

Benign paroxysmal positional vertigo (BPPV) is the most common peripheral vestibular disorder, characterized by transient vertigo episodes triggered by head position changes.1 The most accepted theory for its pathophysiology is the detachment of otoconia from the utricular otolith macula into the semicircular canals (SCC). The horizontal SCC (HSCC) accounts for 5%–30% of all BPPV cases.1,2 HSCC-BPPV can be confirmed with the supine roll test (SRT), where a paroxystic positional nystagmus beating in the plane of the affected canal is evoked, with latency, fatigability, and generally lasting less than 1 min.3 When free otoliths or debris are suspended in the HSCC (canalithiasis), a geotropic or undermost ear direction changing positional nystagmus (DCPN) is observed. Conversely, when these particles are adhered to the cupula (cupulolithiasis), an apogeotropic (uppermost ear) DCPN is observed, with stronger intensity when the head is turned away from the affected ear in the SRT, with brief or no latency, and lasting more than 1 min.3,4
HSCC-BPPV is often a limited disease, nevertheless, there are cases of atypical HSCC-BPPV like heavy and light cupula, that present with common characteristics: persistent DCPN without latency or fatigability, symptoms lasting more than 1 min, and the presence of a null plane.2 The null plane is defined as the position where the nystagmus disappears when the head is rotated during the SRT, and can help identify the affected side in cupulopathy.2 These clinical findings can be explained by a different pathogenesis than for canalithiasis or cupulolithiasis. In heavy cupula this structure has an increased density compared to the endolymph, producing an ampullofugal deflection, with a persistent apogeotropic DCPN.5 In normal conditions the SCC are gravity independent, since the cupula and the endolymph’s gravity is the same, considering they have the same density.6 However, when the cupula’s density becomes lighter or heavier in comparison to the endolymph, its deflection renders it sensitive to gravity.6 Some authors describe heavy cupula to be caused by lighter surrounding endolymph, however, the change in the cupula’s density is the current accepted mechanism, where otolith debris transforms it into a gravity sensitive organ.6 Light and heavy cupula are challenging diagnosis, and their identification can be difficult in the clinical practice.2 Most of these patients have high spontaneous remission with no established treatment.7 This report aims to describe the case of a patient presenting with severe HSCC apogeotropic persistent DCPN.
Case descriptionA 47-year-old premenopausal female patient, with no comorbidities, attends the otolaryngology outpatient consult on July 27th 2019, due to episodic vertigo, triggered by head position changes, during the past week. Vertigo crises were specifically induced after standing from the bed, lasting seconds to minutes, with residual dizziness between crises. Vertigo crises also presented with nausea and vomiting, but no audiologic or neurologic symptoms. The patient recalls a similar clinical presentation two years earlier, however, in that opportunity symptoms were self-limited, and she did not undergo further study.
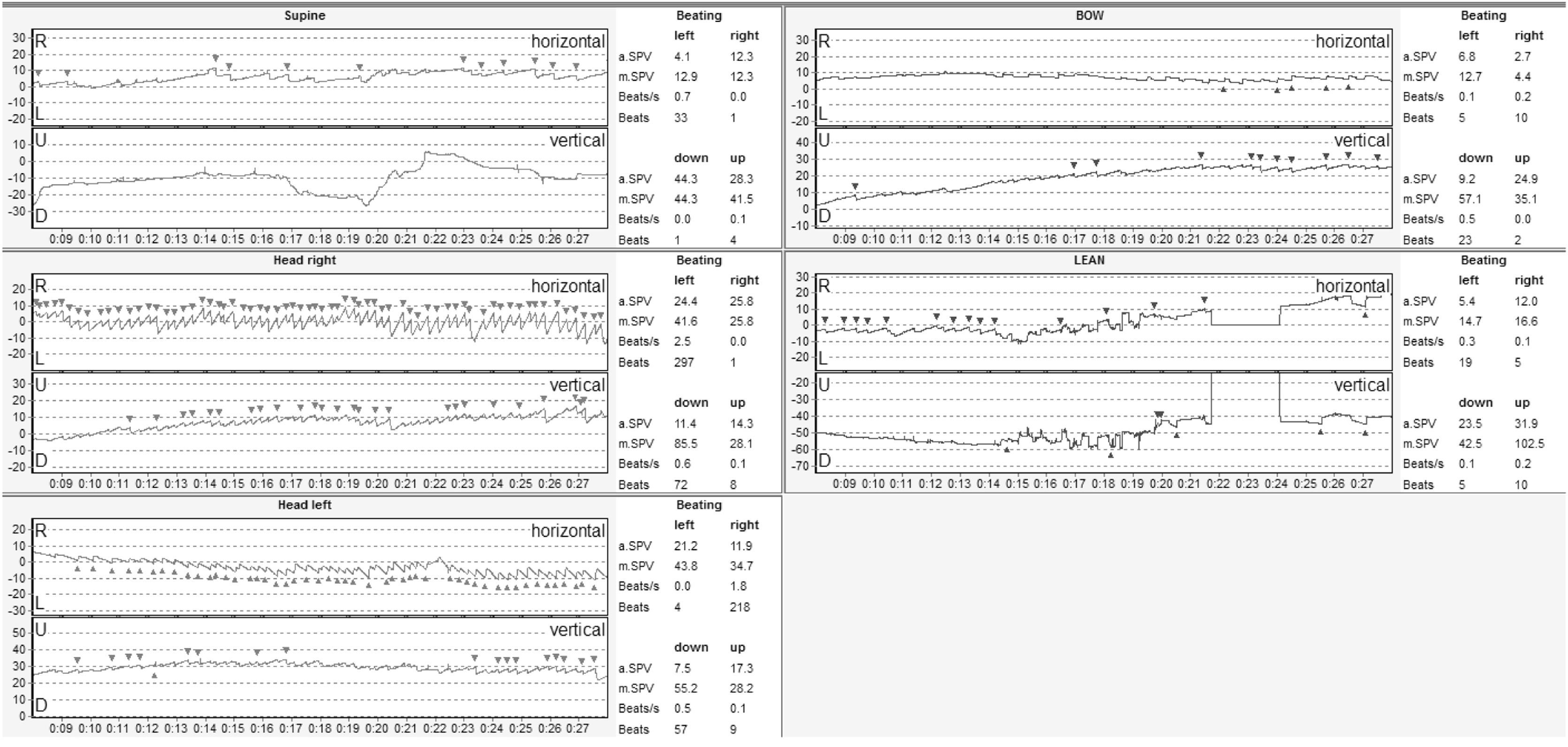
During the physical examination there was no spontaneous nystagmus, a geotropic fatigable horizontal DCPN was found during the SRT, and a horizontal fatigable nystagmus to the left was found during the Dix-Hallpike maneuver to the left. Three days later, a videonystagmography (VNG) showed a spontaneous horizontal nystagmus beating to the right (with reduced intensity during eye fixation). Oculomotor tests were normal. Positional tests with VNG showed an apogeotropic DCPN during the SRT, without latency and more than 4 min duration, of greater intensity when the head turned to the right (Fig. 1A). The Bow and Lean Test showed a horizontal right-beating nystagmus (bow), and then left-beating nystagmus (lean) (Fig. 1B). The caloric test showed a symmetric response. With these results, a HSCC-BPPV was diagnosed, possibly from the left HSCC. Consequently, different repositioning maneuvers were performed in 6 occasions in a 23 day period (first Zuma e Maia; second Gufoni and Zuma e Maia; third Zuma e Maia; finally Zuma e Maia with vibration in 3 different days), yet no improvement was recorded.
 Supine roll test with an apogeotropic DCPN beating with greater intensity and more nystagmic beats when the head turns right. (B) Bow and lean test with right beating horizontal nystagmus during the bow maneuver and left beating nystagmus during the lean maneuver.")
Initial videonystagmography. (A) Supine roll test with an apogeotropic DCPN beating with greater intensity and more nystagmic beats when the head turns right. (B) Bow and lean test with right beating horizontal nystagmus during the bow maneuver and left beating nystagmus during the lean maneuver.
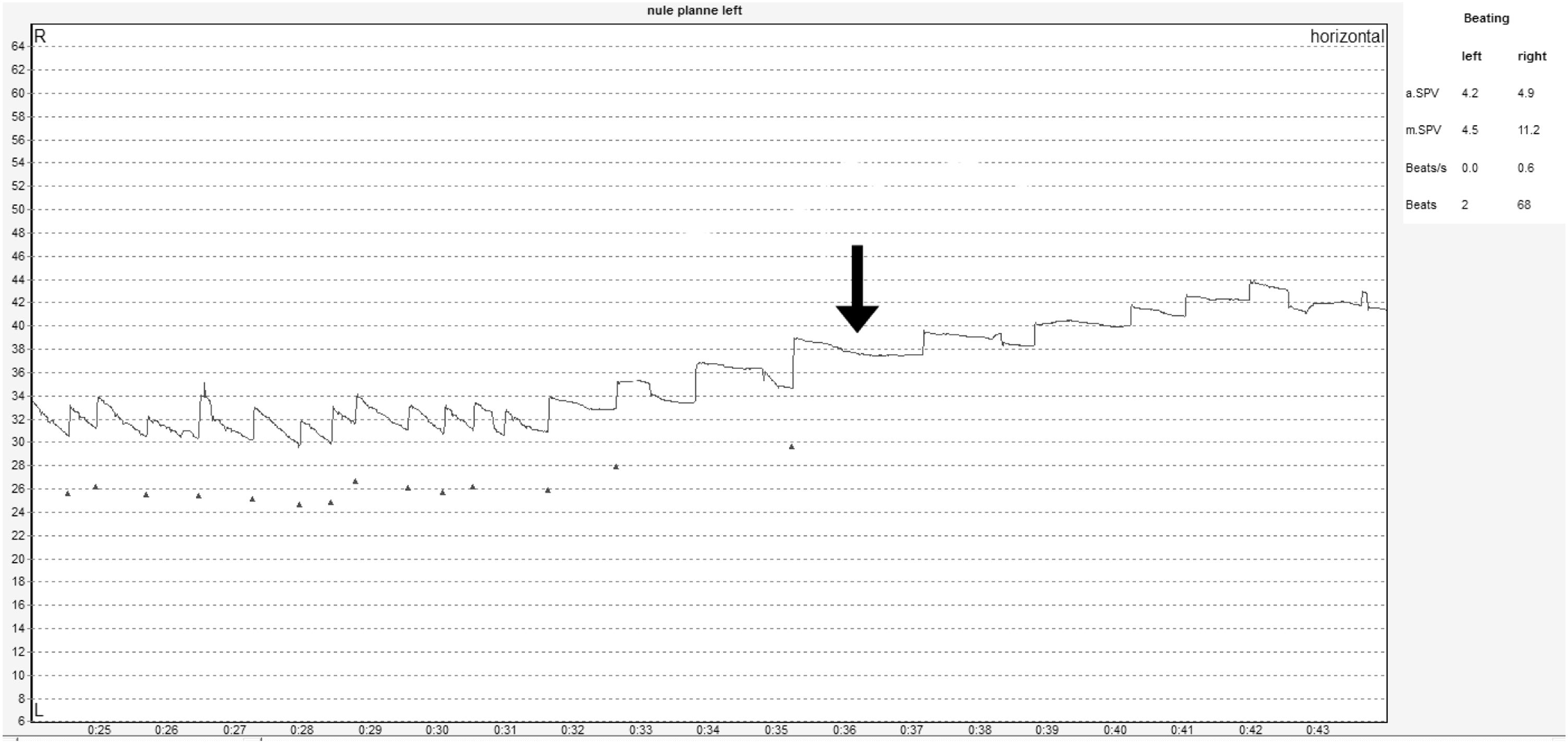
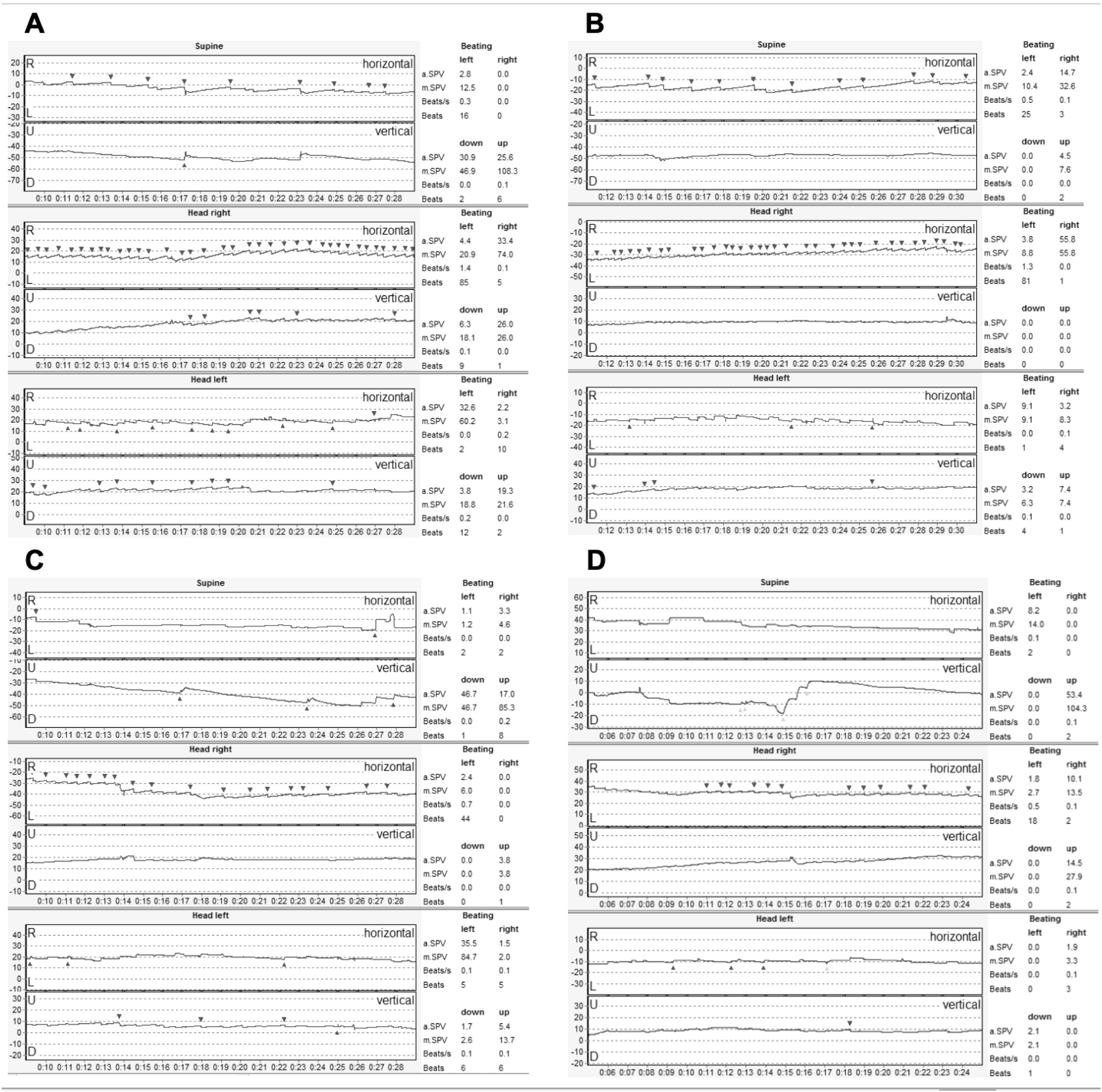
Given the failure with repositioning maneuvers and the persistent positional nystagmus, a null plane was directly sought, identifying it 20° to the left (Fig. 2). This confirmed an atypical HSCC-BPPV: left heavy cupula. An MRI was indicated, ruling out central lesions, and serum 25-hydroxy-vitamin-D was measured, noting a severe deficiency (5.6 ng/mL). A cholecalciferol megadose was prescribed (50,000 UI weekly, during 6-weeks), and subsequently the Zuma e Maia maneuver was performed on 2 occasions immediately after a repeated head-shaking maneuver. Two and three months after the diagnosis, a slight decrease in the nystagmus was observed (Fig. 3A and B). 25-hydroxy-vitamin-D was measured 2-months after the megadose, reaching 66.3 ng/mL. The patient persisted with occasional slight dizziness, accentuated during head position changes, but being able to undergo normal life activities. She was evaluated with a VNG 4 months after the diagnosis, identifying only a mild horizontal apogeotropic DCPN (Fig. 3C). Seven months later, the positional nystagmus completely resolved (Fig. 3D). The patient gave written informed consent, and this manuscript was reviewed and approved by the scientific ethics committee of Pontificia Universidad Católica de Chile (ID: 200630014).

 2-months after the diagnosis, (B) 3-months after the diagnosis, (C) 4-months after the diagnosis, (D) 7-months after the diagnosis, confirming nystagmys resolution.")
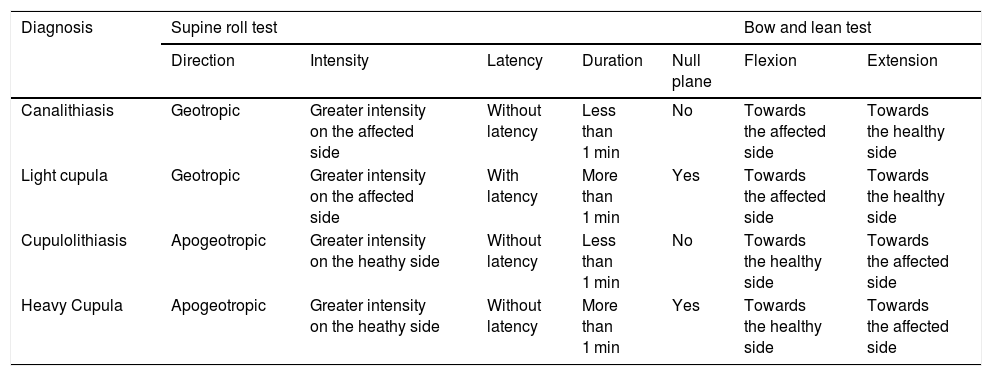
We present a patient with initial geotropic fatigable DCPN, that later changed to apogeotropic persistent DCPN with a null plane at 20° to the left, and initial spontaneous nystagmus beating to the right. The transition from geotropic fatigable DCPN to apogeotropic persistent DCPN could be explained by heavy debris initially in the HSCC, increasing the endolymph density, that later either (1) attaches to the cupula making it heavier, or (2) is followed by an endolymph homeostatic overcompensation, producing a relative increase in the cupula’s density.8 The presence of a spontaneous nystagmus can be seen in both canalithiasis and cupulolithiasis, defined as pseudospontaneous nystagmus.3 This can be observed in an upright head position where a 30° angle inclination between the HSCC and the horizontal gravity plane places the ampulla at a higher position than the rest of the canal.3 This causes deflection of the ampulla away from the utricle in heavy cupula cases, resulting in nystagmus beating towards the healthy ear.2 Differential diagnosis should be made with cupulolithiasis in the presence of apogeotropic nystagmus, and canalithiasis in the presence of geotropic nystagmus (Tables 1 and 2).2,3 Central lesions must be ruled out in patients presenting with cupulopathy, given the persistent character of the DCPN, which can also occur in central lesions.6
Differential diagnosis findings during examination.
| Diagnosis | Supine roll test | Bow and lean test | |||||
|---|---|---|---|---|---|---|---|
| Direction | Intensity | Latency | Duration | Null plane | Flexion | Extension | |
| Canalithiasis | Geotropic | Greater intensity on the affected side | Without latency | Less than 1 min | No | Towards the affected side | Towards the healthy side |
| Light cupula | Geotropic | Greater intensity on the affected side | With latency | More than 1 min | Yes | Towards the affected side | Towards the healthy side |
| Cupulolithiasis | Apogeotropic | Greater intensity on the heathy side | Without latency | Less than 1 min | No | Towards the healthy side | Towards the affected side |
| Heavy Cupula | Apogeotropic | Greater intensity on the heathy side | Without latency | More than 1 min | Yes | Towards the healthy side | Towards the affected side |
Differential diagnosis according to direction of nystagmus.
| Apogeotropic persistent DCPN | Geotropic persistent DCPN | |
|---|---|---|
| Differential diagnosis | Cupulolithiasis | Canalithiasis |
| Heavy cupula | Light cupula | |
| Pseudo nystagmus | Nystagmus beats towards the healthy side | Nystagmus beats towards the affected side |
The torpid evolution with no or little response to repositioning maneuvers during 2–3 months, and complete resolution after 7 months is noteworthy. BPPV is usually treated with particle repositioning maneuvers, nevertheless, in atypical BPPV these maneuvers may not be as efficient, hence vestibular suppressants should be prescribed.5 Most studies state there are no effective treatment options. Some authors advocate repositioning maneuvers, although spontaneous remission within first weeks is frequent,4 while more severe cases have been described to last 2 months.4 On the other hand, Tang et al.2 report 16 patients with heavy cupula diagnosis, treated with the Barbecue maneuver, or Gufoni and then Barbecue maneuvers. Treatment failure was seen in 3 patients at 7 days and only 1 patient after 30 days. However, these patients may have presented spontaneous resolution.
The accurate localization of the affected side is fundamental for improved treatment outcomes. In heavy cupula, this can be identified by the nystagmus’ intensity, the Bow and Lean test, and the null plane position2 (Table 1). The presence of null points in patients with persistent DCPN may indicate a gravity sensitive cupulophathy,6 and the position varies greatly, with a standard deviation of 22.4° in heavy cupula.4 In the present case, multiple repeated repositioning maneuvers failed to resolve the vertigo and nystagmus, and 2 months after the diagnosis, only a reduction in the nystagmus had been achieved. After this, no more repositioning maneuvers were performed, and the patient evolved positively with a reduction in symptoms intensity.
Additionally, the patient’s serum 25-hydroxy-vitamin-D levels were normalized as symptoms decreased. Many studies have tried to establish the relation between vitamin D deficiency and BPPV. To date, an association has been demonstrated between vitamin D deficiency and more severe symptoms, a longer duration, a lower success rate of repositioning maneuvers and a higher recurrence rate.9 This could explain the treatment failure in the present case. On the other hand, studies have proven that patients with canalithiasis have lower 25-hydroxy-vitamin-D levels than patients with cupulolithiasis.10 In the present cupulopathy case, the patient had a severe vitamin D deficiency. More studies are required to clearly establish the difference between vitamin D levels in canalithiasis and cupulolithiasis, and to determine the possible pathophysiology for this finding. It is unclear whether this patient’s symptoms resolved due to natural history, and/or the cholecalciferol megadose.
ConclusionsBPPV is a frequent cause of vertigo, yet its atypical forms may present a defying diagnosis and treatment. When faced with an atypical BPPV with failure to treatment, a null plane must be sought, and central lesions must be ruled out. The affected side should be accurately localized in order to improve the treatment outcomes. This patient presented a challenging treatment and her symptoms resolved after 7 months.
FundingThis study did not require funding.
Conflicts of interestThe authors declare no conflicts of interest.
Peer Review under the responsibility of Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial.


