

Benign paroxysmal positional vertigo (BPPV) is the most common cause of peripheral vestibular dysfunction.
ObjectiveTo assess whether the performance of the Dix–Hallpike maneuver after the Epley positioning maneuver has prognostic value in the evolution of unilateral ductolithiasis of posterior semicircular canal.
MethodsA prospective cohort study in monitored patients at otoneurology ambulatory with a diagnosis of BPPV; they were submitted to the therapeutic maneuver and then to a retest in order to evaluate the treatment effectiveness; all cases were reassessed one week later and the retest prognostic value was evaluated.
ResultsA sample of 64 patients which 47 belonging to negative retest group and 17 belonging to positive retest. Performed the maneuver in all patients, the retest presented 51.85% sensitivity, 91.89% specificity, 82.35% positive predictive value and 72.34% negative predictive value.
ConclusionThe study shows that doing the retest after repositioning maneuver of particles in BPPV is effectual, since it has high specificity.
A vertigem posicional paroxística benigna (VPPB) é a causa mais comum de disfunção vestibular periférica.
ObjetivoAvaliar se a realização do reteste de Dix-Hallpike após a manobra de posicionamento de Epley tem valor prognóstico na evolução da vertigem posicional da ductolitíase paroxística benigna de canal semicircular posterior unilateral.
MétodoEstudo prospectivo do tipo coorte de pacientes em acompanhamento no ambulatório de otoneurologia com diagnóstico de VPPB; foram submetidos a manobra terapêutica e posteriormente ao reteste para avaliar a eficácia do tratamento; todos os casos foram reavaliados em uma semana e analisado o valor prognostico do reteste.
ResultadosAmostra de 64 pacientes, 47 do grupo reteste negativo e 17 do reteste positivo; realizada manobra de Epley em todos os pacientes. O reteste apresentou sensibilidade de 51,85%; especificidade de 91,89%; valor preditivo positivo de 82,35% e valor preditivo negativo de 72,34%.
ConclusãoO estudo mostra que é válido realizar o reteste após a manobra de reposicionamento de partículas na VPPB, visto que possui alta especificidade.
BPPV is caused by otoconial debris coming from utricular macula, moving to one or more semicircular canals and mistakenly stimulating the ampullary crest.1
Positional nystagmus is essential to establish the diagnosis of BPPV. Through the characteristics of the nystagmus, it is possible to identify the affected semicircular canal and damaged labyrinth, and a distinction between cupulolithiasis and canalithiasis also can be drawn. Thus, the most appropriate treatment can be implemented.2
Performing specific maneuvers for otolith repositioning in the treatment of BPPV has attracted special interest, due to its ease of applicability and good results. Such maneuvers are aimed at removing theotoconial debris situated into the ducts or semicircular canal cupulae toward the vestibule, following an ampulifugal movement.3 Considering that the debris scattered through the endolymph has a higher density than that of the surrounding endolymph, it can be moved noninvasively by means of a sequence of orientations of the head relative to gravity.4
The literature informs us that there is variability in the results on the number of repositioning maneuvers necessary for the abolition of positional nystagmus.5 Some studies suggest an average of 1.23 maneuvers,6 others, 1.36 maneuvers,7 and in a more recent study, 1.53 maneuvers.4
In clinical practice, some doctors perform a Dix–Hallpike maneuver retest shortly after otolith repositioning, as a strategy to predict treatment success. However, there is no data showing whether this assessment is valuable as a routine.
Given the paucity of data in the literature, this study aimed to assess whether the implementation of a retest for the Dix–Hallpike maneuver after Epley positioning had prognostic value in the evolution of benign paroxysmal positional vertigo by unilateral posterior semicircular canal canalolithiasis.
MethodsThis is a prospective cohort study, approved by the Research Ethics Committee (opinion number 200,813), which included 64 patients from the otoneurology department each with clinical picture characteristic of benign paroxysmal positional vertigo (BPPV). All study participants signed an informed consent.
Patients with impairment of the lateral or anterior semicircular canal, nystagmus lasting for more than a minute (which characterizes cupulolithiasis), signs or symptoms of central nervous system involvement, bilateral involvement of posterior semicircular canal, physical restrictions that prevented performing the diagnostic or therapeutic maneuver, and patients with only dizziness and with no positional nystagmus on the diagnostic maneuver were excluded from the study. Patients who were using anti-vertigo drugs up to 3 days and benzodiazepines up to 5 days before the study were also excluded from the study. Patients diagnosed with unilateral posterior canal BPPV, who had dizziness and positional nystagmus with latency duration <1min and fatigability to Dix–Hallpike maneuver were included.
At the first visit, an oriented history, a complete physical otorhinolaryngologic and otoneurologic examination and a positioning nystagmus test were performed. All cases were evaluated by the same examiner. The diagnostic maneuver performed was the Dix–Hallpike test: in the sitting position, the patient has the head turned 45° toward the side which to be tested; and then the patient is laid down backwards. At the end of the maneuver, the patient's head is slightly extended and turned toward the tested side.1 The test was initiated by the opposite position to the triggering position of vertigo and/or nystagmus, according to information obtained from each patient.
After identifying the semicircular canal involved (by triggering nystagmus position and direction), all patients underwent the Epley repositioning maneuver. In this maneuver, the patient is placed in the Dix–Hallpike maneuver position, which triggers positional nystagmus, maintaining this position for 1–2min. Next, the patient's head is slowly driven, with the aid of the hands of the examiner, up to an inclination of 45° toward the opposite side; during this step, the patient moves his/her body in the same direction and way, assuming a lateral decubitus position. The head movement in the same direction and way continues until the patient's nose is pointing to 45° downwards. This position is maintained by the patient for another 1–2min. Finally, the patient returns slowly to the sitting position, facing the opposite side from the beginning of the maneuver.7
After about 10min of the procedure, the patient was subjected to the retest, which consists in another positioning maneuver (Dix–Hallpike). The retest was considered positive only if the nystagmus was present in the triggering position. The retest was considered negative if the patient was asymptomatic, or even if recounting dizziness without clinical evidence of nystagmus.
The patients were subdivided into two groups: group I, patients with negative retest; and group II, patients with positive retest. The patients were evaluated for age and number of maneuvers required.
One week after the repositioning maneuver, all patients were reassessed and submitted again to Dix–Hallpike maneuver, to evaluate whether or not an improvement of their clinical condition occurred; improvement was considered complete if the patient was asymptomatic and had no nystagmus during the maneuver.
Statistical analysis was performed with the program SPSS for Windows – version 10.0; numeric data were presented as mean±standard deviation and categorical data as percentages. The comparison between the two groups of numerical data was performed using the Mann–Whitney test and, for categorical data, the chi-squared test was used, with a significance level set at p<0.05. Retest sensitivity, specificity, positive predictive value and negative predictive value retest were calculated.
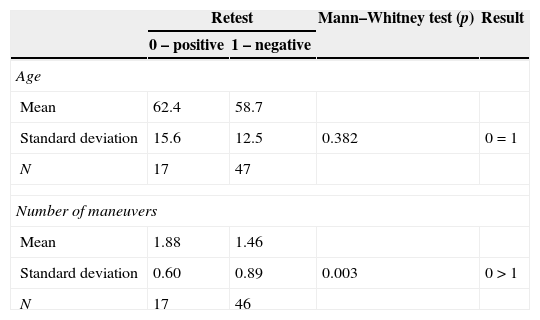
ResultsThe study sample consisted of 64 patients diagnosed with BPPV, 47 (73.4%) in the retest-negative group and 17 (26.5%) in the retest-positive group. The mean age was 58.7 years (SD±12.5) for group I and 62.4 years (SD±15.6) for group II. Most patients were female in both group I (55.3%) and in group II (58.8%) (Tables 1 and 2).
The mean number of maneuvers required to achieve a favorable result with complete improvement in our overall sample was 1.56; group I needed 1.46 maneuvers and group II, 1.88 maneuvers, a statistically significant difference (p=0.003).
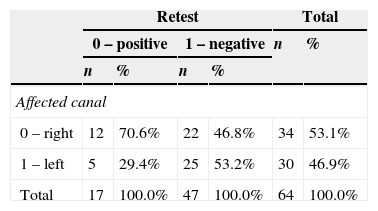
Considering all patients, the right side was the more affected (53.1% of the entire sample); there was no statistically significant difference between groups.
Considering the Dix–Hallpike maneuver as the gold standard, the retest showed a sensitivity of 51.85%; specificity of 91.89%; positive predictive value of 82.35% and negative predictive value of 72.34%. The false-negative rate was 48.15% and the false-positive rate was 8.11% (Table 3).
DiscussionOver the years, there have been attempts to predict the success of maneuvers for treatment of BPPV; in cases of BPPV of the posterior semicircular canal, the results of repositioning can be predicted by the characteristics of the induced nystagmus during the Epley maneuver; the importance of the pattern of nystagmus in the second position of the Epley maneuver (90° contralateral to the initial position of the head) is well recognized. In this position, nystagmus with characteristics similar to the original position would suggest a successful repositioning of particles.8
Repetitive therapeutic maneuvers in a single session have been proposed, until nystagmus was no longer seen or until vertigo and nystagmus disappearance; some authors suggest that the treatment of BPPV through repetition of Epley maneuvers in a single session proved to be more efficient than a single maneuver per session.9
The repetition of the Dix–Hallpike (retest) maneuver after the Epley maneuver, in an attempt to predict the success of treatment, has not been described in the literature. It is assumed that, if the retest results positive, there is a great likelihood of patient returning in the next week with no resolution of the problem.
In this study, patients were divided into two groups: group I and group II, with negative and positive retest, respectively; these groups showed homogeneity regarding sex and age. There was a predominance of females in this sample, with a mean age of 59.7 years. Several studies have suggested a higher incidence in women,9–11 but in younger patients and in those cases secondary to trauma, the incidence may be equal between men and women. The age of onset falls most commonly between the fifth and seventh decades.10–12 The elderly are in increased risk; a study in a population of elderly patients undergoing geriatric assessment for complaints unrelated to equilibrium found that 9% had undiagnosed BPPV.13
The mean number of maneuvers of the sample was 1.56; in general literature, on average 1.23 maneuvers14; 1.366; 1.315; and 1.3816 were observed. According to Vrabec,7 the number of repositioning maneuvers needed to induce BPPV remission is variable, and multiple treatments may be needed for more than one third of patients.10 Based on these data, conducting the retest after the Epley maneuver was not a harmful procedure, since there was no increase in the average number of maneuvers required. Comparing the number of maneuvers, with the use of the Mann–Whitney test between groups there was a statistically significant greater number of maneuvers in group II; this result was expected, given that, theoretically, these patients would not have a good response with a single maneuver.
The right posterior semicircular canal was the most affected in this population; several studies have shown that the right ear is predominantly affected by BPPV. It was demonstrated that the side affected by BPPV correlates with the preferred position on the bed. In the right lateral decubitus position, the openings of both posterior and lateral right channels are in a lower position, which facilitates the entry of heavy particles from the utricle. Thus, one can speculate that BPPV predominantly involves the right ear, because many people prefer to sleep on the right side, possibly due to a nagging feeling of heart beats when lying on the left side.11
Procedure tolerance was considered good in both groups; only one patient had nausea and vomits while performing the retest. Another study, which conducted several Epley maneuvers in the same session, also demonstrated good tolerability; transient nausea and imbalance were the only symptoms immediately reported.17
In all 64 patients in the present study, no case of conversion from posterior to anterior horizontal semicircular canal was observed, even when the Dix–Hallpike maneuver had been repeated in the same day; one study observed approximately 15.9% conversion to another channel, and all cases occurred in patients who underwent a new Dix–Hallpike maneuver. These authors suggest that a period of time in the vertical position would be required to allow that those not fully repositioned particles to move out of the common crus area, reducing the risk of re-entry; thus, for these authors, a 15-min interval would reduce substantially the incidence of subsequent reentry.12 In our study, a range of approximately 10min between the Epley maneuver and retesting was allowed, with no case of conversion to other channels.
In our study, the retest showed low sensitivity (51.85%) and high specificity (91.89%), a positive predictive value of 82.35% and a negative predictive value of 72.34%. Thus, if the retest has a positive result, one can assume that the particles of calcium carbonate were not properly repositioned. This finding demonstrates the importance of a positive retest, since it will help to differentiate patients who are unlikely to have a quick resolution of BPPV, and thus will depend on a larger number of maneuvers. Thus, in cases of positive retest, a new repositioning maneuver can be performed in the same visit. On the other hand, if a negative result of the retest was obtained, one cannot infer that the patient will return with or without improvement of his/her condition.
The finding that a negative retest does not completely accurately predict the success of BPPV treatment can be explained by several reasons.
First, the nystagmus observed in BPPV is prone to fatigue with repeated attempts to provocation, and its absence may not mean particle repositioning.14
Another hypothesis would be the incomplete return of otoconial debris into the vestibule, leaving some particles in the posterior canal, which could not be sufficient to reach the threshold and trigger nystagmus and/or vertigo (negative retest). In the following week, these fragments would form new clusters, again achieving the required threshold to generate vertigo with nystagmus. Otoconial particles were studied intraoperatively, showing that it is the binding of those small fragments that will form a large conglomerate. Thus, this conglomerate may break up during the Epley maneuver. Some of the particles would flow into the utricle, and the others would flow back into the posterior canal ampulla.15 The remaining debris would not be sufficient to divert the cupule and reach the needed threshold level to stimulate the vestibular-ocular route.16 The calcium carbonate particles can be clustered into various sizes, or dispersed through the semicircular canal. Presumably, patients requiring additional maneuvers have more dispersed particles into smaller masses. These masses are removed more slowly through repeated maneuvers; and, at each maneuver, these masses probably become even more widespread in the utricle. Thus, they may not be sufficient to trigger the nystagmus.
A rate of 8.1% false-positives, i.e., patients who showed a positive retest but were found asymptomatic the following week, was found. These patients may have presented a spontaneous remission in this time interval, resulting mainly from the ability of the endolymph to dissolve otoconia displaced by its low ionized calcium content (20mM), resulting in the disappearance of BPPV symptoms.18 Thus, during the Epley maneuver, there would be a fragmentation of otoconia and a larger portion would have stayed in the duct, triggering nystagmus and dizziness while the retest was being conducted; in the following week, this material would have been reabsorbed by endolymph.
ConclusionThe study shows the importance of conducting a retest after a maneuver of particle repositioning in patients with BPPV, since this procedure has high specificity. Thus, when faced with a patient with a positive retest, one can infer that there is a great likelihood of the patient returning in the next week with no improvement; and one can also suggest performing more Epley maneuvers in the same session, when the retest comes positive.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Oliveira AK, Suzuki FA, Boari L. Is it important to repeat the positioning maneuver after the treatment for benign paroxysmal positional vertigo? Braz J Otorhinolaryngol. 2015;81:197–201.
Institution: Instituto de Assistência Medica ao Servidor Público Estadual de São Paulo, São Paulo, SP, Brasil.
gology is pleased to honor the reviewers


