

Cleft lip and/or palate (CL/P) represent the most common congenital anomalies of the face.
ObjectiveTo evaluate the prevalence of depressive symptoms in children and adolescents with nonsyndromic cleft lip and/or palate (nsCL/P).
MethodsWe conducted an observational, case-control study, with a case study group composed of 61 patients with nsCL/P, aged 7–17 years, and a control group of 61clinically normal patients. Both groups were selected at the same institution.
ResultsDepressive symptoms were observed in the case group (nsCL/P), but there were no statistically significant differences compared to the control group. No association was found between the two groups (case and control) in relation to sociodemographic variables: gender, age and education.
ConclusionsThis study identified the prevalence of depressive symptoms in children and adolescents with nsCL/P from a localized geographic population, although the results were not statistically significant when compared to the control group, not justifying the use of CDI (Child Depression Inventory) as a screening instrument for depressive symptoms in the examined population.
Fissuras labiais e/ou palatinas (FL/Ps) representam as anomalias craniofaciais mais comuns.
ObjetivosAvaliar a prevalência de sintomas depressivos em crianças e adolescentes não sindrômicos com FL/P (FL/PNS).
MétodoFoi realizado um estudo observacional de caso-controle com uma amostra populacional de conveniência, com um grupo caso (61 pacientes com FL/PNS, tendo idades entre 7 a 17 anos) e um grupo controle (61 pacientes clinicamente normais). Ambos os grupos foram selecionados na mesma Instituição.
ResultadosSintomas depressivos foram observados no grupo caso (FL/PNS), mas não houve diferenças estatisticamente significantes quando comparado com o grupo controle. Não foi encontrada associação entre os dois grupos (caso e controle) em relação às variáveis sociodemográficas: gênero, idade e educação.
ConclusõesEste estudo observou a prevalência de sintomas depressivos em crianças e adolescentes com FL/PNS de uma população geográfica localizada, embora os resultados não tenham sido estatisticamente significantes quando comparado com o grupo controle, não justificando assim a utilização do Inventário de Depressão Infantil (IDI), como instrumento rastreador de sintomas depressivos na população analisada.
Nonsyndromic lip and/or palate cleft (NSCL/P) is the most prevalent congenital genetic defect of craniofacial area and results in anatomical complications and in psychological and behavioral disorders.1 The incidence of NSCL/P varies according to geographic location, race and socioeconomic status,2,3 and has a mean distribution of about 1 case per 700 live births.4 The etiology of NSCL/P is multifactorial, involving several genes and complex molecular events that occur during embryogenesis, that are also influenced by environmental factors.5,6
Some studies have suggested an increased risk for the development of psychiatric disorders in children and adolescents with NSCL/P, and have noted abnormal levels of depressive symptoms.7–12 The literature contains population-based studies that identify depressive disorders in the general population, that reach a prevalence of 10% and an incidence of 2%.13 It is estimated that approximately 5% of people worldwide have depression, and about 10–25% of them may show some depressive episode during life.14,15
The prevalence of depression in childhood increases with age, and is approximately 2% overall; it increases progressively and at adolescent ages, reaches levels close to adulthood.16 In different regions of the world, including Brazil, these values range from 0.4 to 3.0% for children, and 3.3 to 12.4% for teenagers. These variations can be explained by methodological differences in sample selection strategy, as well as by cultural differences, depending on where the studies have been conducted.15–17
Early detection of depressive symptoms could indicate social, school or family environment damage,7,8,18 and, therefore, several methods are used for screening and diagnosis.19,20 The Child Depression Inventory (CDI) is used to assess depressive symptoms in children and adolescents in different clinical and research contexts.19–21 Thus, some studies have shown an association between occurrence of this malformation and psychosocial adjustment, suggesting greater attention to patients with NSCL/P, including their overall development and integration with the social environment.21–24
In addition, psychiatric and psychological support of patients with NSCL/P throughout growth and development and also throughout the entire period of rehabilitation is necessary, in order to understand the needs of patients and of their parents who are feeling and living with a craniofacial malformation.10,11,23,24 Thus, the aim of this study was to assess the prevalence of depressive symptoms in children and adolescents with NSCL/P.
MethodsWe conducted a case–control observational study. All participants were selected from the same institution (Centro de Referência para Reabilitação de Anomalias Craniofaciais e Clínicas Odontológicas e Médicas), in Minas Gerais, Brazil. The case study group consisted of 61 patients with NSCL/P, all of them children and teenagers between the ages of 7 and 17; the control group consisted of 61 clinically healthy individuals (with negative personal or family history for craniofacial changes or syndromes), in the same case group. Both groups were selected by chance, enrolling an adequate number of subjects to equal the previous sampling calculations used to determine the number of subjects needed for statistical purposes. Patients with CL/P as one manifestation of a clinical syndrome and those with a family history of consanguinity were excluded from the study. We compared the prevalence and severity of depressive symptoms between groups by applying CDI, a self-directed and self-explanatory questionnaire.19
This instrument (CDI) (Table 1) was developed in order to detect the presence and severity of depressive symptoms in children and adolescents so as to identify changes in mood, self worth, vegetative functions and self-evaluative and interpersonal behaviors. The 27 items of this questionnaire are summed to obtain a score that can be validated and specifically reflect the nationality of the questionnaire.19,25 During the application of the questionnaire, each item of CDI was read in the presence of the patients to ensure understanding and remove uncertainties. The alpha value was set at 0.5%. A cut off point (score) of 17 points had been previously established for statistical significance. The results were compared using the chi-squared test and by logistic regression analysis. This study was approved by the Institutional Ethics Committee (N°. 56/2010).
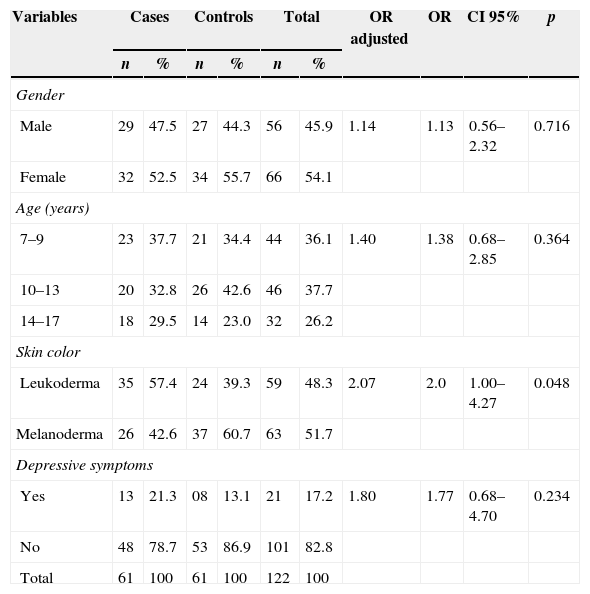
ResultsThe distribution of case (n=61) and control (n=61) groups followed a normal pattern for gender, and in both groups the most prevalent age was between 7 and 13 years (Table 2). When the classification of NSCL/P was evaluated for the case group, we found a higher frequency of cleft palate (n=33), with equal distribution for isolated cleft lip and palate (n=14; corresponding to 23% for each in the group). When the two groups were compared, the logistic regression analysis identified no association among sociodemographic variables: gender (p=0.716; OR 1.14; CI 95% 0.56–2.32), age (p=0.364; OR 1.40; CI 95% 0.68–2.85) and schooling (p=0.082; OR 3.34; CI 95% 0.86–13.0). An association was detected for skin color (p=0.048; OR 3.34; CI 95% 1.0–4.27), meaning that individuals with NSCL/P are 3.34 times more likely to be Caucasians (Table 2).
General characteristics of patients with nonsyndromic lip and palate clefts (case group) and without lip and palate clefts (control group).
| Variables | Cases | Controls | Total | OR adjusted | OR | CI 95% | p | |||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||||
| Gender | ||||||||||
| Male | 29 | 47.5 | 27 | 44.3 | 56 | 45.9 | 1.14 | 1.13 | 0.56–2.32 | 0.716 |
| Female | 32 | 52.5 | 34 | 55.7 | 66 | 54.1 | ||||
| Age (years) | ||||||||||
| 7–9 | 23 | 37.7 | 21 | 34.4 | 44 | 36.1 | 1.40 | 1.38 | 0.68–2.85 | 0.364 |
| 10–13 | 20 | 32.8 | 26 | 42.6 | 46 | 37.7 | ||||
| 14–17 | 18 | 29.5 | 14 | 23.0 | 32 | 26.2 | ||||
| Skin color | ||||||||||
| Leukoderma | 35 | 57.4 | 24 | 39.3 | 59 | 48.3 | 2.07 | 2.0 | 1.00–4.27 | 0.048 |
| Melanoderma | 26 | 42.6 | 37 | 60.7 | 63 | 51.7 | ||||
| Depressive symptoms | ||||||||||
| Yes | 13 | 21.3 | 08 | 13.1 | 21 | 17.2 | 1.80 | 1.77 | 0.68–4.70 | 0.234 |
| No | 48 | 78.7 | 53 | 86.9 | 101 | 82.8 | ||||
| Total | 61 | 100 | 61 | 100 | 122 | 100 | ||||
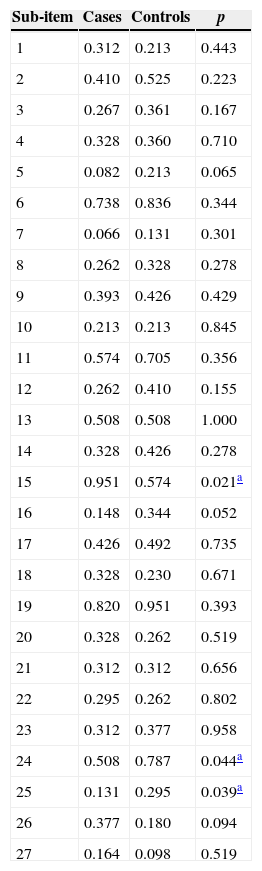
We detected the presence of depressive symptoms in 21.3%, n=13 of the case group (NSCL/P); however, there was no statistical significance compared to the control group (p=0.234, OR 1.80, 95% CI 0.68–4.70) (Table 2). The analysis of each of the 27 items of CDI identified a homogeneous distribution for the frequency of depressive symptoms in both groups. An association for three items was observed, when we compared the mean of scores, by CDI sub-items (Table 3). Concerning the item related to suicide, it was observed that 8.4% (n=5) of subjects in the case group (nsL/PC) reported some suicidal thoughts compared to only 1.6% (n=1) in the control group.
Comparison of mean scores by sub-item of CDI (p-value, comparison of medians by Kruskal–Wallis test) of patients with nonsyndromic lip and palate cleft (case group) and control patients (n=122).
| Sub-item | Cases | Controls | p |
|---|---|---|---|
| 1 | 0.312 | 0.213 | 0.443 |
| 2 | 0.410 | 0.525 | 0.223 |
| 3 | 0.267 | 0.361 | 0.167 |
| 4 | 0.328 | 0.360 | 0.710 |
| 5 | 0.082 | 0.213 | 0.065 |
| 6 | 0.738 | 0.836 | 0.344 |
| 7 | 0.066 | 0.131 | 0.301 |
| 8 | 0.262 | 0.328 | 0.278 |
| 9 | 0.393 | 0.426 | 0.429 |
| 10 | 0.213 | 0.213 | 0.845 |
| 11 | 0.574 | 0.705 | 0.356 |
| 12 | 0.262 | 0.410 | 0.155 |
| 13 | 0.508 | 0.508 | 1.000 |
| 14 | 0.328 | 0.426 | 0.278 |
| 15 | 0.951 | 0.574 | 0.021a |
| 16 | 0.148 | 0.344 | 0.052 |
| 17 | 0.426 | 0.492 | 0.735 |
| 18 | 0.328 | 0.230 | 0.671 |
| 19 | 0.820 | 0.951 | 0.393 |
| 20 | 0.328 | 0.262 | 0.519 |
| 21 | 0.312 | 0.312 | 0.656 |
| 22 | 0.295 | 0.262 | 0.802 |
| 23 | 0.312 | 0.377 | 0.958 |
| 24 | 0.508 | 0.787 | 0.044a |
| 25 | 0.131 | 0.295 | 0.039a |
| 26 | 0.377 | 0.180 | 0.094 |
| 27 | 0.164 | 0.098 | 0.519 |
Some studies have reported an increased risk for the development of psychiatric disorders in children and adolescents with NSCL/P, citing abnormally high levels of depressive symptoms.10,11,26–28 A meta-analysis that included 340 studies identified high levels of depressive symptoms in several chronic diseases or conditions, in comparison with normal individuals.28 Marked differences were found in chronic fatigue syndrome, fibromyalgia, migraine, epilepsy and in CL/P. The presence of these symptoms was more prevalent in female patients and in individuals living in developing countries.28 In the present study, despite the presence of depressive symptoms in the case group with NSCL/P (21.3%, n=13), no positive statistical significance was observed, when compared with control group (p=0.234; OR 1.80; CI 95% 0.68–4.70). A stratified analysis showed no association of depressive symptoms in both groups (case versus control) in the combination of variables, such as gender (p=0.145) and age (p=0.165).
It is known that the early detection of depressive symptoms is important for identifying in advance any ill-effects on the family, social and school environments7,8,26–28 so that the application of screening and diagnotic methods can guide the treatment of these patients.19,29 In an Irish case–control study, the authors compared the presence of functional, psychological disorders, such as anxiety and depression, and also behavioral disorders, among 160 children and adolescents with NSCL/P and in 113 normal individuals.30 An important association of changes in behavior and depressive symptoms in the presence of NSCL/P (p<0.001) was observed. In our study, a score of 17 was used, based on the adaptation and standardization of this instrument in Brazil.26 The analysis of each of the 27 items of CDI identified a homogeneous distribution of the frequency of depressive symptoms in both groups, thus with no positive association. In the Irish study, with respect to facial appearance and difficulty with speech, patients were more unhappy than controls, and high suicide rates were observed, as in our study, with 8.4% (n=5) of the respondents in the case group (NSCL/P), compared with 1.6% (n=1) in the control group.30 Another study found a high incidence of psychological disorders and difficulties with social interaction in patients with CL/P.10
With respect to cleft type, we found higher rates of problems related to anxiety, depression, and learning and speech difficulties in children with isolated palate cleft, compared to children with both lip and palate cleft.31 In the present study, when comparing the presence of depressive symptoms among patients in the case group (NSCL/P) versus control group, we found similarities with those results, but with no positive statistical correlation. Other studies also point to an association between the occurrence of this malformation and psychosocial adjustment, suggesting greater attention to patients with NSCL/P, including their overall development and integration into the social environment.29,32–35Although this study was conducted in a referral center for rehabilitation of craniofacial anomalies, it has some limitations, such as the limited geographic area, i.e., restricted to a portion of a single Brazilian state. For all analyzes, alpha was 0.05. The sample size was sufficient for the detection of a difference of two points between groups in CDI instrument, considering a coefficient of variation of 0.5 and a statistical power of 0.8.
Although our results do not confirm the findings in the literature, this study suggests that psychological and psychiatric support is needed for patients with NSCL/P throughout their growth and development, and throughout the rehabilitation period, in order to understand the needs of patients and of their families who are experiencing first hand a craniofacial malformation.7,8,18,35 We also need to emphasize that in a limited geographic area and with the methodology and tool chosen, the use of a screening instrument for depressive symptoms for this group of individuals with NSCL/P was not justifiable.10,11,23,24 Thus, the aim of this study was to assess the prevalence of depressive symptoms in children and adolescents with NSCL/P.
ConclusionThe authors of this study identified the prevalence of depressive symptoms in children and adolescents with nsCL/P from a localized geographic population, although the results were not statistically significant compared with the control group. There was no association of depressive symptoms with sociodemographic variables (gender, age and schooling). CDI is an instrument used in various chronic clinical and genetic conditions, aimed to identify patients with the potential or the risk of developing depressive symptoms. But in the specific population of the present study, we did not feel it necessary to adopt CDI as a screening instrument for such craniofacial abnormalities.
Conflicts of interestThe authors declare no conflicts of interest.
This study was supported by Fundação de Amparo à Pesquisa do Estado de Minas Gerais – FAPEMIG; Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPq; Procad/Casadinho – CNPq/Capes.
Please cite this article as: Lima LS, Ribeiro GS, de Aquino SN, Volpe FM, Martelli DR, Swerts MS, et al. Prevalence of depressive symptoms in patients with cleft lip and palate. Braz J Otorhinolaryngol. 2015;81:177–83.
Institution: Postgraduate Program in Health Sciences, Centro de Ciências Biológicas e da Saúde, Universidade Estadual de Montes Claros (UNIMONTES), Montes Claros, MG, Brazil.
gology is pleased to honor the reviewers


