
Solitary plasmacytoma is a rare malignant tumor of plasma cells with no evidence of systemic proliferation. There are two known subtypes: extramedullary solitary plasmacytoma and solitary bone plasmacytoma. The etiology is still unknown. Both lesions present a risk of progression to multiple myeloma. A number of approaches have been used for treatment of solitary plasmacytoma.
ObjectiveTo carry out a systematic review of the case reports described in the literature, focusing on therapeutic and prognostic aspects.
MethodsA search of clinical case reports was performed in the PubMed database using Mesh Terms related to “plasmacytoma” under the following criteria: type of study (case report), articles in English language, conducted in humans, with no publication date limits.
ResultsOf the 216 articles found, only 21 articles met the pre-established inclusion criteria.
ConclusionThe occurrence of solitary bone plasmacytoma in the bones of the face is a rare condition prevalent between the 4th and 6th decades of life, located in the posterior region of the mandible in most cases. Histopathological examination and systemic investigation are mandatory for confirmation of diagnosis.
O plasmocitoma solitário é um tumor maligno raro de células plasmáticas sem evidência de proliferação sistêmica e engloba dois subtipos: plasmocitoma solitário extramedular e plasmocitoma solitário ósseo. A etiologia ainda é desconhecida. Ambas as lesões apresentam risco de progressão para mieloma múltiplo. Uma série de abordagens tem sido usada para seu tratamento.
ObjetivoRealizar uma revisão sistemática da literatura com enfoque nos aspectos terapêuticos e prognósticos.
MétodoRealizou-se uma busca de relatos de caso clínico na base de dados PubMed com termos de busca relacionados com “plasmocitoma” sob os seguintes critérios: tipo de estudo (relato de caso), artigos na língua inglesa, estudos realizados apenas em humanos, sem limites de data de publicação.
ResultadosDos 216 artigos encontrados, apenas 21 artigos preencheram os critérios de inclusão pré-estabelecidos.
ConclusãoA ocorrência de plasmocitoma solitário ósseo nos ossos da face é uma condição rara prevalente entre a 4a e a 6a décadas de vida, localizada na região posterior de mandíbula na maioria dos casos. O exame histopatológico e a investigação sistêmica são mandatórios para confirmação do diagnóstico.
Solitary plasmacytoma (SP) is a rare malignant tumor of plasma cells with no evidence of systemic proliferation. When there is systemic involvement, that is, the involvement of multiple skeletal sites, the disease is called multiple myeloma (MM), one of the most frequent presentations of neoplasia of the plasma cells.1
The SP presents an incidence of 2–5% of all neoplasms and two subtypes: extramedullary solitary plasmacytoma (ESP) and solitary bone plasmacytoma (SBP).1,2 ESP originates from soft tissues and is more frequent in the head and neck region, specifically in the upper respiratory tract, whereas the SBP presents as an intramedullary bone lesion in the axial skeleton or pelvic bones.3
The etiology of solitary plasmacytoma is unknown, however, it is suggested that chronic stimulation, radiation overdose, viral infections and genetic interaction in the reticuloendothelial system may contribute to the development of the lesion.4
The SBP has a predilection for males between the 6th and the 7th decades of life, however, it can affect individuals of any age. Patients affected by SBP, in general, present a primary complaint of swelling associated with minimal pain.5,6
The SBP can present two radiographic patterns: the first can be a delimited radiolucent area; the second, as a destructive lytic mass in the mandible. Microscopically, monoclonal proliferation of plasmacytoid cells with eccentric nuclei and basophilic cytoplasm are observed.7,8
Once the biopsy is performed and the histopathological diagnosis of SBP is defined, it is important to submit the patient to systemic investigation of disseminated disease through imaging examinations of the whole body, bone marrow biopsy, complete hematological examination and electrophoresis of urine and plasma to screen proteins synthesized by tumor cells.1,9–11
Although MM is a relatively common occurrence when compared to other plasma cell neoplasms, SBP in the skull bones is a relatively rare entity with very little published literature.12 The objective of the present study is to perform a systematic review of case reports focusing on its epidemiology, clinical and microscopic characteristics, as well as its diagnosis, treatment, prognosis and the importance of longitudinal clinical follow-up.
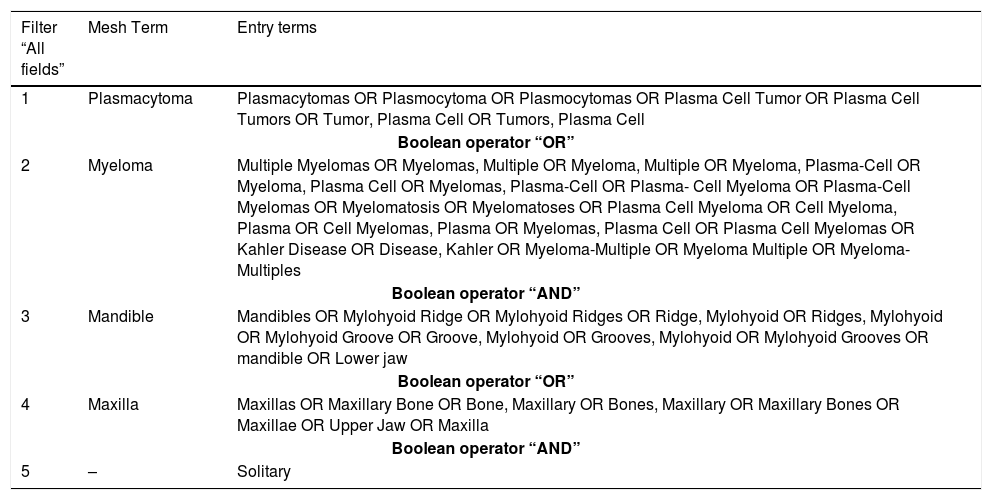
MethodsA systematic review of the case reports was performed from articles found in the PubMed/MEDLINE database. A search strategy was developed using the Pubmed Advanced Search Builder with the following combinations of the Mesh terms “Plasmacytoma”, “Myeloma”, “mandible” and “maxilla” and the derived entry terms in conjunction with the Boolean operators “OR” And “AND”, as described in Table 1. The inclusion criteria applied for the case reports were: type of study (case reports), in English language and conducted in humans.
Search strategy on Pubmed Advanced Search Builder.
| Filter “All fields” | Mesh Term | Entry terms |
|---|---|---|
| 1 | Plasmacytoma | Plasmacytomas OR Plasmocytoma OR Plasmocytomas OR Plasma Cell Tumor OR Plasma Cell Tumors OR Tumor, Plasma Cell OR Tumors, Plasma Cell |
| Boolean operator “OR” | ||
| 2 | Myeloma | Multiple Myelomas OR Myelomas, Multiple OR Myeloma, Multiple OR Myeloma, Plasma-Cell OR Myeloma, Plasma Cell OR Myelomas, Plasma-Cell OR Plasma- Cell Myeloma OR Plasma-Cell Myelomas OR Myelomatosis OR Myelomatoses OR Plasma Cell Myeloma OR Cell Myeloma, Plasma OR Cell Myelomas, Plasma OR Myelomas, Plasma Cell OR Plasma Cell Myelomas OR Kahler Disease OR Disease, Kahler OR Myeloma-Multiple OR Myeloma Multiple OR Myeloma-Multiples |
| Boolean operator “AND” | ||
| 3 | Mandible | Mandibles OR Mylohyoid Ridge OR Mylohyoid Ridges OR Ridge, Mylohyoid OR Ridges, Mylohyoid OR Mylohyoid Groove OR Groove, Mylohyoid OR Grooves, Mylohyoid OR Mylohyoid Grooves OR mandible OR Lower jaw |
| Boolean operator “OR” | ||
| 4 | Maxilla | Maxillas OR Maxillary Bone OR Bone, Maxillary OR Bones, Maxillary OR Maxillary Bones OR Maxillae OR Upper Jaw OR Maxilla |
| Boolean operator “AND” | ||
| 5 | – | Solitary |
Based on the search strategy, 216 articles were found. Applying the inclusion criteria as filter, 114 articles were excluded. The remaining 102 articles were submitted to selective reading of the titles, which determined the exclusion of 78 articles. The remaining 24 articles were submitted to analysis of the abstracts and, at this stage, three articles were excluded because they presented SP lesion located in an anatomical region distinct from the oral and maxillofacial surgeons’ expertise.
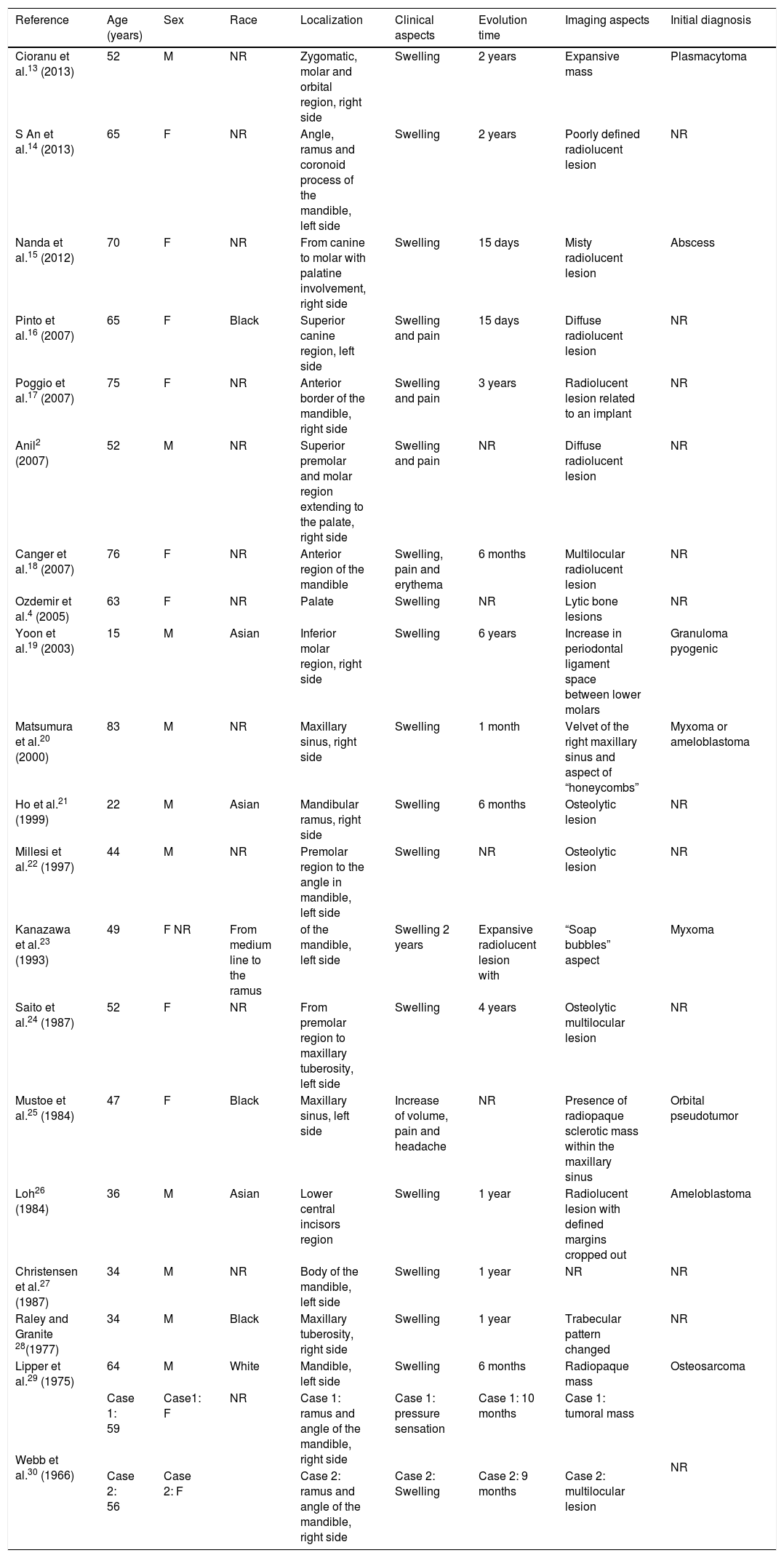
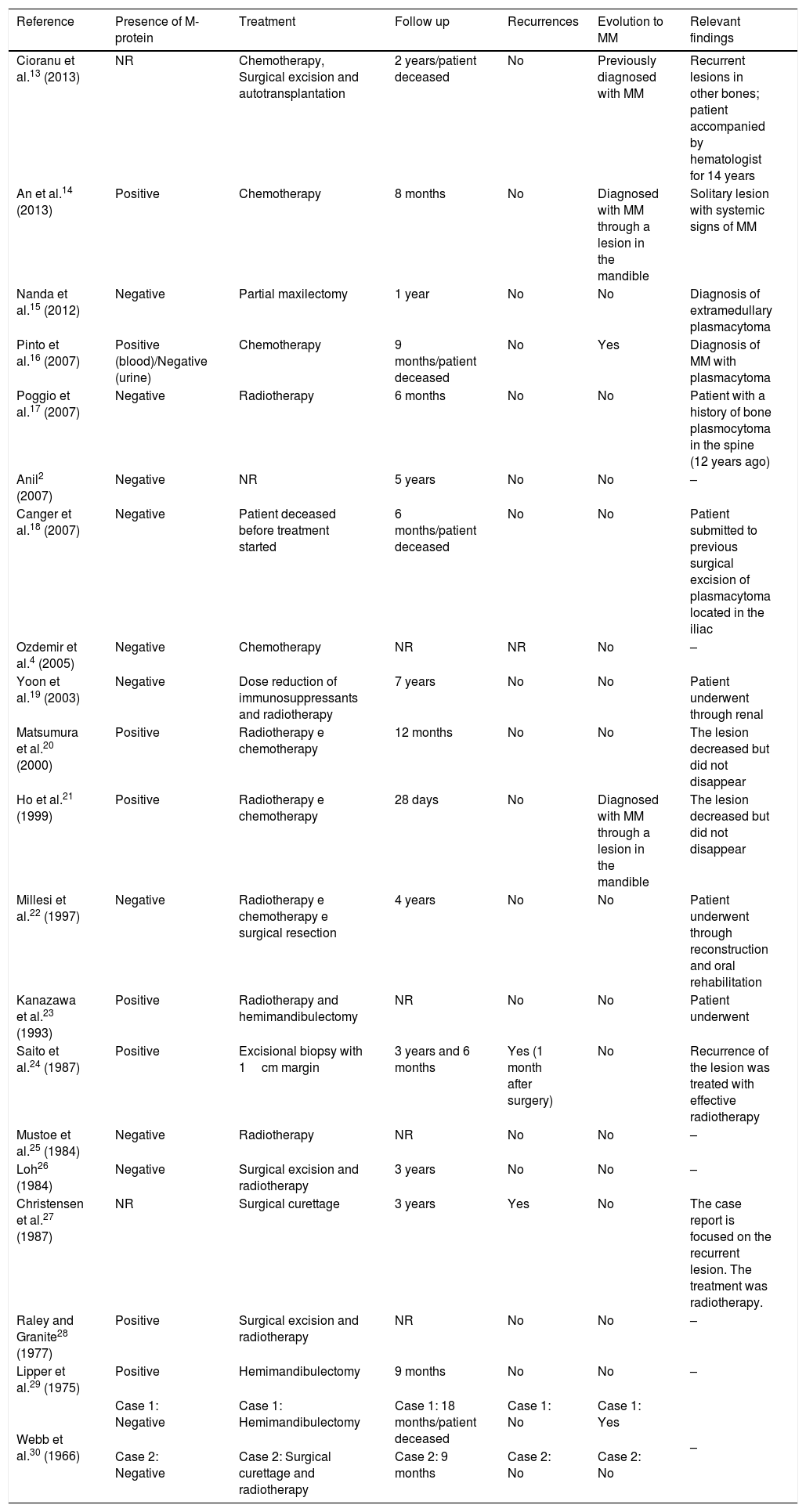
The interpretative reading of the full case reports was carried out in 21 articles: 20 case reports and 1 case series. The case reports were arranged in descending order of the year of publication in two tables: one providing epidemiological and clinical data as well as the initial diagnosis (Table 2); the other (Table 3) containing information regarding the detection of M-protein (or paraprotein), therapeutic approach, follow-up time, recurrences and evolution for MM, as well as findings considered relevant to each article. In addition, the case series was included in the discussion of this same study.
Epidemiological and clinical data.
| Reference | Age (years) | Sex | Race | Localization | Clinical aspects | Evolution time | Imaging aspects | Initial diagnosis |
|---|---|---|---|---|---|---|---|---|
| Cioranu et al.13 (2013) | 52 | M | NR | Zygomatic, molar and orbital region, right side | Swelling | 2 years | Expansive mass | Plasmacytoma |
| S An et al.14 (2013) | 65 | F | NR | Angle, ramus and coronoid process of the mandible, left side | Swelling | 2 years | Poorly defined radiolucent lesion | NR |
| Nanda et al.15 (2012) | 70 | F | NR | From canine to molar with palatine involvement, right side | Swelling | 15 days | Misty radiolucent lesion | Abscess |
| Pinto et al.16 (2007) | 65 | F | Black | Superior canine region, left side | Swelling and pain | 15 days | Diffuse radiolucent lesion | NR |
| Poggio et al.17 (2007) | 75 | F | NR | Anterior border of the mandible, right side | Swelling and pain | 3 years | Radiolucent lesion related to an implant | NR |
| Anil2 (2007) | 52 | M | NR | Superior premolar and molar region extending to the palate, right side | Swelling and pain | NR | Diffuse radiolucent lesion | NR |
| Canger et al.18 (2007) | 76 | F | NR | Anterior region of the mandible | Swelling, pain and erythema | 6 months | Multilocular radiolucent lesion | NR |
| Ozdemir et al.4 (2005) | 63 | F | NR | Palate | Swelling | NR | Lytic bone lesions | NR |
| Yoon et al.19 (2003) | 15 | M | Asian | Inferior molar region, right side | Swelling | 6 years | Increase in periodontal ligament space between lower molars | Granuloma pyogenic |
| Matsumura et al.20 (2000) | 83 | M | NR | Maxillary sinus, right side | Swelling | 1 month | Velvet of the right maxillary sinus and aspect of “honeycombs” | Myxoma or ameloblastoma |
| Ho et al.21 (1999) | 22 | M | Asian | Mandibular ramus, right side | Swelling | 6 months | Osteolytic lesion | NR |
| Millesi et al.22 (1997) | 44 | M | NR | Premolar region to the angle in mandible, left side | Swelling | NR | Osteolytic lesion | NR |
| Kanazawa et al.23 (1993) | 49 | F NR | From medium line to the ramus | of the mandible, left side | Swelling 2 years | Expansive radiolucent lesion with | “Soap bubbles” aspect | Myxoma |
| Saito et al.24 (1987) | 52 | F | NR | From premolar region to maxillary tuberosity, left side | Swelling | 4 years | Osteolytic multilocular lesion | NR |
| Mustoe et al.25 (1984) | 47 | F | Black | Maxillary sinus, left side | Increase of volume, pain and headache | NR | Presence of radiopaque sclerotic mass within the maxillary sinus | Orbital pseudotumor |
| Loh26 (1984) | 36 | M | Asian | Lower central incisors region | Swelling | 1 year | Radiolucent lesion with defined margins cropped out | Ameloblastoma |
| Christensen et al.27 (1987) | 34 | M | NR | Body of the mandible, left side | Swelling | 1 year | NR | NR |
| Raley and Granite 28(1977) | 34 | M | Black | Maxillary tuberosity, right side | Swelling | 1 year | Trabecular pattern changed | NR |
| Lipper et al.29 (1975) | 64 | M | White | Mandible, left side | Swelling | 6 months | Radiopaque mass | Osteosarcoma |
| Webb et al.30 (1966) | Case 1: 59 | Case1: F | NR | Case 1: ramus and angle of the mandible, right side | Case 1: pressure sensation | Case 1: 10 months | Case 1: tumoral mass | NR |
| Case 2: 56 | Case 2: F | Case 2: ramus and angle of the mandible, right side | Case 2: Swelling | Case 2: 9 months | Case 2: multilocular lesion |
Detection of M-protein (or paraprotein), therapeutic approach, follow-up time, recurrences and evolution for MM, as well as findings considered relevant to each article.
| Reference | Presence of M-protein | Treatment | Follow up | Recurrences | Evolution to MM | Relevant findings |
|---|---|---|---|---|---|---|
| Cioranu et al.13 (2013) | NR | Chemotherapy, Surgical excision and autotransplantation | 2 years/patient deceased | No | Previously diagnosed with MM | Recurrent lesions in other bones; patient accompanied by hematologist for 14 years |
| An et al.14 (2013) | Positive | Chemotherapy | 8 months | No | Diagnosed with MM through a lesion in the mandible | Solitary lesion with systemic signs of MM |
| Nanda et al.15 (2012) | Negative | Partial maxilectomy | 1 year | No | No | Diagnosis of extramedullary plasmacytoma |
| Pinto et al.16 (2007) | Positive (blood)/Negative (urine) | Chemotherapy | 9 months/patient deceased | No | Yes | Diagnosis of MM with plasmacytoma |
| Poggio et al.17 (2007) | Negative | Radiotherapy | 6 months | No | No | Patient with a history of bone plasmocytoma in the spine (12 years ago) |
| Anil2 (2007) | Negative | NR | 5 years | No | No | – |
| Canger et al.18 (2007) | Negative | Patient deceased before treatment started | 6 months/patient deceased | No | No | Patient submitted to previous surgical excision of plasmacytoma located in the iliac |
| Ozdemir et al.4 (2005) | Negative | Chemotherapy | NR | NR | No | – |
| Yoon et al.19 (2003) | Negative | Dose reduction of immunosuppressants and radiotherapy | 7 years | No | No | Patient underwent through renal |
| Matsumura et al.20 (2000) | Positive | Radiotherapy e chemotherapy | 12 months | No | No | The lesion decreased but did not disappear |
| Ho et al.21 (1999) | Positive | Radiotherapy e chemotherapy | 28 days | No | Diagnosed with MM through a lesion in the mandible | The lesion decreased but did not disappear |
| Millesi et al.22 (1997) | Negative | Radiotherapy e chemotherapy e surgical resection | 4 years | No | No | Patient underwent through reconstruction and oral rehabilitation |
| Kanazawa et al.23 (1993) | Positive | Radiotherapy and hemimandibulectomy | NR | No | No | Patient underwent |
| Saito et al.24 (1987) | Positive | Excisional biopsy with 1cm margin | 3 years and 6 months | Yes (1 month after surgery) | No | Recurrence of the lesion was treated with effective radiotherapy |
| Mustoe et al.25 (1984) | Negative | Radiotherapy | NR | No | No | – |
| Loh26 (1984) | Negative | Surgical excision and radiotherapy | 3 years | No | No | – |
| Christensen et al.27 (1987) | NR | Surgical curettage | 3 years | Yes | No | The case report is focused on the recurrent lesion. The treatment was radiotherapy. |
| Raley and Granite28 (1977) | Positive | Surgical excision and radiotherapy | NR | No | No | – |
| Lipper et al.29 (1975) | Positive | Hemimandibulectomy | 9 months | No | No | – |
| Webb et al.30 (1966) | Case 1: Negative | Case 1: Hemimandibulectomy | Case 1: 18 months/patient deceased | Case 1: No | Case 1: Yes | – |
| Case 2: Negative | Case 2: Surgical curettage and radiotherapy | Case 2: 9 months | Case 2: No | Case 2: No |
The distribution of SBP cases by age ranged from 15 to 83 years, with a mean age of 54.15 years for both sexes, 43.6 years for men and 61.54 years for women. The highest incidence of SBP occurred between the 4th and 6th decades of life.2,4,13–30 The distribution by gender was balanced, accounting for 11 cases in women and 10 in men. These data corroborate the results obtained by Dores et al.12
The patient's race was reported in only 7 case reports: 3 black patients, 3 Asian patients and 1 white patient.2,4,13–30 Although most of the case reports did not report the race of the patients, a predilection of the SBP for white individuals is observed in the literature.12
Location of the lesionIn the case reports reviewed, the most common site of SBP appearance was the mandible, more precisely in posterior regions.2,4,13–30 These findings confirm those found by Loh26 and Pisano et al.31
Although the literature presents pain as the main symptom.2 The present study found painless increase in volume as the most common clinical finding. Headache and pressure sensation have also been reported.25,30 The time of evolution of the lesion ranged from 15 days to 72 months, with an average time of evolution of 15.11 months.2,4,13–31
Imaging aspects and initial diagnosisRadiographically, it was observed that, in most studies, the solitary plasmacytoma appears as a diffuse, multilocular radiolucent lesion. Bone destruction seems to be limited to the medullary region of the skull bones.2,4,13–30
Only 8 case reports presented a presumptive clinical diagnosis, and the hypotheses presented were: abscess, pyogenic granuloma, myxoma, ameloblastoma, orbital pseudotumor and osteosarcoma.13,15,19,20,23,25,26,29
Differential diagnosis of PBS should be performed in relation to other lesions that are similar in the routine imaging exams such as ameloblastoma, keratocystic odontogenic tumor, myxoma, giant cell central lesion, metastatic tumors, vascular malformation, sarcoma and lymphoma.32,33 Thus, the histopathological examination becomes essential for the definitive diagnosis.
Presence of M-proteinPlasma protein M or paraprotein, monoclonal immunoglobulin synthesized by tumor cells, was investigated in 18 cases.2,4,13–30 The presence of the M-protein was reported in 8 case reports,14,16,20,21,23,24,28,29 corresponding to 38.09%. This rate is in the range of 24–72% indicated in other studies.5
The presence of M-protein is obtained by examination of electrophoresis from blood or urine samples.33 The use of this exam to determine the diagnosis of SBP is still inexact since the presence of paraprotein does not always determine the existence of the disease in question, however, it should be emphasized that its diagnostic value is relevant in cases where it is desired to evaluate the presence of M-protein.1,34
There are authors who advocate that the presence of paraprotein even after treatment may be indicative of residual tumor or hidden.1,35
TreatmentThe treatment used for the cases were the following:
- •
Only radiotherapy – 2 cases.17,25
- •
Only chemotherapy – 3 cases.4,14,16
- •
Only surgical intervention – 5 cases.5,24,27,29,30
- •
Surgical intervention associated to radiotherapy – 4 cases.23,26,28,30
- •
Radiotherapy associated to chemotherapy – 2 cases.20,21
- •
Surgical intervention, radiotherapy and autotransplantation – 1 case.13
- •
Radiotherapy and decreased dosage of immunosuppressors – 1 case.19
- •
Radiotherapy, chemotherapy and surgical intervention – 1 case.22
In one of the case reports the therapeutic approach was not reported2 and in an other, the patient deceased before starting treatment.18 The ideal therapeutic approach is still controversial, however, radiotherapy seems to be the treatment that offers better clinical results since the SBP reveals itself as a radiosensitive lesion.5,36 The rates of local control of SBP with radiotherapy presented in the literature exceed the range of 80%.2,37,38 Surgical intervention should be carried out in situations where there is no prediction of functional or esthetic damage.23
Chemotherapy is advocated only on the basis of reports in the literature that showed improvement of local control and delayed development of MM.38 However, chemotherapy alone has no benefit compared to radiotherapy but when instituted adjunctively it appears to offer beneficial effect in patients with a higher risk of treatment failure, that is, those with tumor lesions greater than 4–5cm.1,38,39
Prognosis and follow-upFollow-up time after treatment ranged from 28 days to 7 years. The mean follow-up period was 19.9 months. There were 4 deaths.13,16,18,19
In only 2 cases (9.5%) did SBP evolve to MM.16,30 The low incidence of progression to MM in skull bones damage was reported in the same way in other retrospective studies.23,26
Frequently, SBP can be found as a radiographic finding and can represent a primary lesion or focus of MM as previously reported.40,41 The present study revealed that in 2 case reports, MM was diagnosed from the detection of a skull bone lesion.14,21
There were 2 reports of recurrence of the lesion, and in one case the event occurred in 1 month and in another after 3 years, both treated surgically.24,27 The mean time to recurrence of lesion after treatment reported in other studies was 2–2.5 years.42
The worst prognosis corresponds to progression from SBP to MM. Such event is directly related to the size of the tumors. Scientific evidence suggests that patients who present tumor masses, previously diagnosed as SBP, with a size larger than 4–5cm have a higher risk of developing MM.39 In addition, the bone location of the plasmacytoma in comparison with the extramedullary entity, age (patients over 60 years) and the presence of paraprotein at the time of diagnosis also determine higher progression rates for MM.36,43
Final considerationsSBP is a rare condition in the bones of the face. It affects patients between the 4th and 6th decades of life without predilection for gender. The lesion arises mainly in the mandible, more precisely in the posterior region. Commonly, it presents as a multilocular radiolucent lesion. The main sign associated with the development of SBP is painless volume increase. Biopsy and histopathologic examination are mandatory since the definition of diagnosis determines the need for advanced investigation to rule out the possibility of MM.
The importance of early diagnosis is justified in that the plasmacytoma may be a primary or metastatic lesion of MM. The treatment of choice for SBP is radiotherapy. The association of surgical intervention and chemotherapy is reserved for specific cases. Periodic follow-up of the patient is necessary for at least 3 years after diagnosis due to the possibility of developing MM.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Lombardo EM, Maito FL, Heitz C. Solitary plasmacytoma of the jaws: therapeutical considerations and prognosis based on a case reports systematic survey. Braz J Otorhinolaryngol. 2018;84:790–8.
Peer Review under the responsibility of Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial.
gology is pleased to honor the reviewers


