
Lung cancer usually spreads by lymphatic or hematogenous route; around one fifth of newly diagnosed lung adenocarcinomas present with distant metastases in organs such as brain, adrenal glands, liver and bones.1 However, lung cancer metastases in the temporal bone are quite rare, and as such, present substantial diagnostic challenge. Clinical manifestations of metastatic disease in the temporal bone are usually obscure and may include symptoms such as hearing loss, tinnitus, vertigo, facial palsy, otalgia, otorrhea and headache. The occurrence of an osteolytic lesion in the temporal bone (even in the absence of a known primary tumor) should always be considered as a possible metastasis, especially in elderly patients. The authors present a rare case of an otogenic facial palsy and metastasis in the temporal bone as an initial manifestation of lung cancer and discuss potential diagnostic pitfalls. This paper was approved by the Ethics Committee of Clinic for Otorhinolaryngology and Maxillofacial Surgery.
Case reportA 73-year-old female patient presented with peripheral facial palsy and otalgia that were treated for about two months in a primary health care center. After an incomplete resolution of symptoms, the patient was admitted into our facility for additional diagnostics and follow-up. Otomicroscopic examination on the left ear revealed hyperemic tympanic membrane with prominent pars flaccida. Patient also had left periphery facial palsy (House-Brackmann scale, grade 3), conductive left hearing loss (air bone gap 30dB), B-type tympanometry, high rate of C-reactive protein (60mg/L) and leukocytosis (14×106L−1). Patient had normal body temperature, and was without nausea or dizziness. According to medical record, patient was treated for chronic obstructive bronchitis and osteoporosis, with regular controls and follow-up.
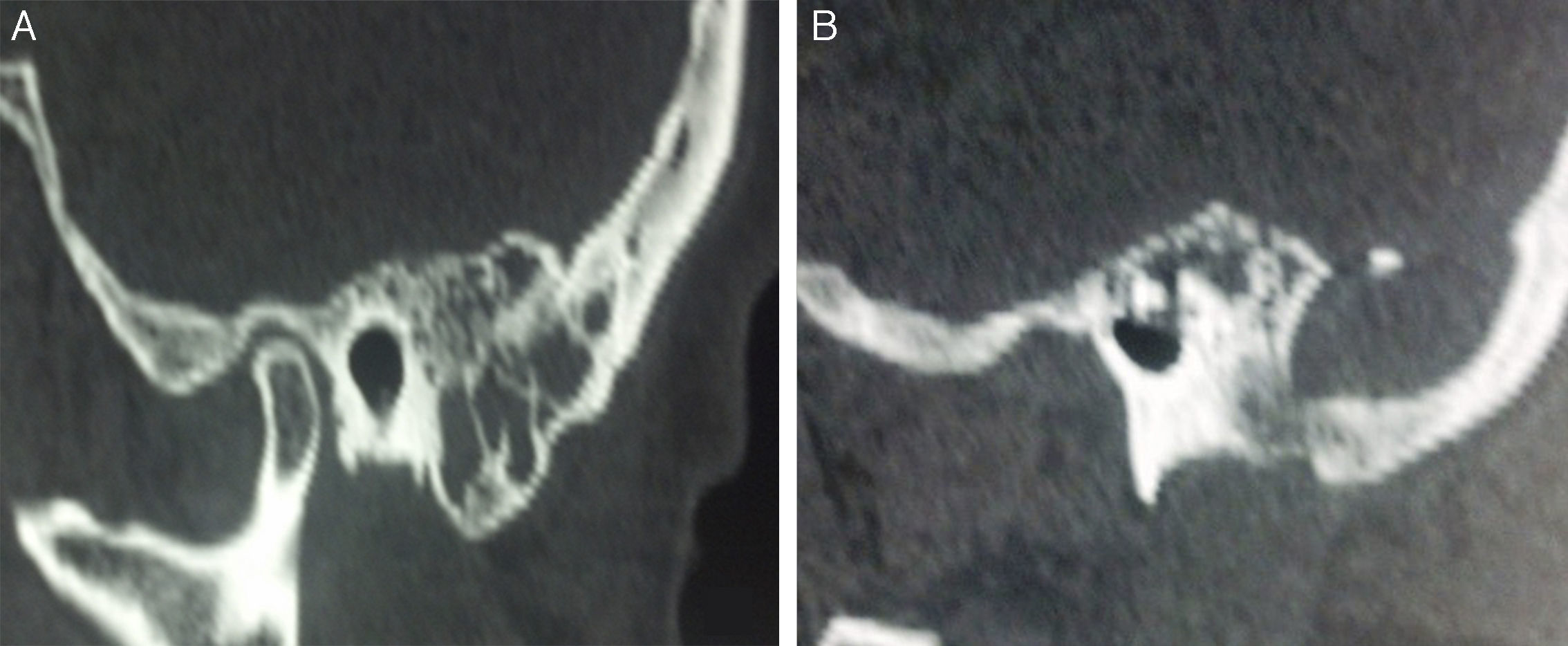
Temporal bone computed tomography (CT) revealed mucosal thickening within the mastoid air cells, osteolytic lesion in the left mastoid and occipital bone and the heterogeneous mass in the middle ear structures (Fig. 1). Treatment with intravenous antibiotics ensued (Ceftriaxone 2g/per day), without any improvement of symptoms. Patient had no signs or symptoms of the malignant disease; chest radiography showed no signs of lung cancer.
 Temporal bone CT scan: thickened mucosa within the mastoid air cells. (B) Presence of an expansive osteolytic temporal bone lesion; note the destruction of mastoid apex.")
During surgery, the mastoidectomy, paracenthesis and ventilation tube implantation were performed. We noted presence of soft, friable, granulation tissue in the antrum and in the mastoid; fragments were sent for histopathological analysis.
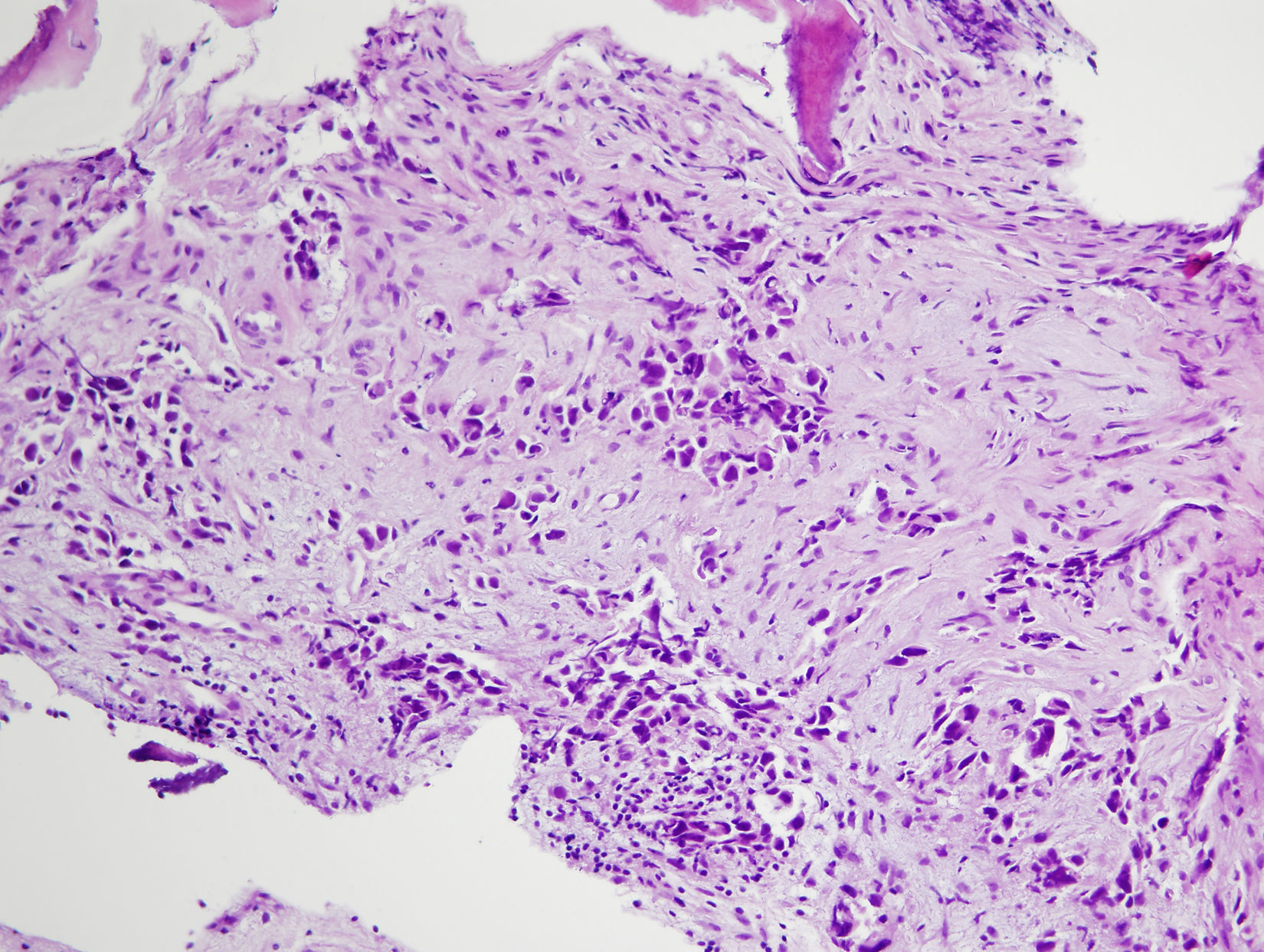
Histopathological and immunohistochemical analysis revealed presence of rare atypical cells that were cytokeratin- and TTF-1 positive (Fig. 2). Therefore, the case was diagnosed as the metastasis of lung carcinoma. Chest CT scan, bronchoscopy and histopathological analysis of lung samples ensued; these additional analyses confirmed the diagnosis of a lung adenocarcinoma that was localized in the apical segment of the left lung. In a very short period of time, our patient–who at the time also had bilateral mediastinal lymph node enlargement–died suddenly, prior to any specific oncological treatment.
Discussion
Metastases in the temporal bone are relatively rare; the most common primary sites usually are breast, lung, kidney and stomach cancers.2–5 The pattern of metastatic spread toward the temporal bone may involve lymphatic/hematogenous route, diffuse metastatic leptomeningeal carcinomatosis or direct extension of tumor.2 Lung cancer usually spreads via hematogenous route, in head and neck region usually toward brain.1,2,5 In our case, metastatic spread was due to lymphatic/hematogenous spread of tumor cells that also caused mediastinal lymphadenopathy. Due to hematogenous spread, tumor cell emboli may favor the petrous apex of the temporal bone, which has bone marrow that is irrigated by a slow-flow capillary network.
Clinical examination of patients with temporal bone metastasis may show various findings, such as retroauricular soft tissue swelling or swelling of the tissue structures in the external auditory canal, inflammation (such as otitis media with effusion), perforation of tympanic membrane, otalgia, facial paralysis and several others; in some cases, metastasis in the temporal bone may even be without symptoms.6,7
Facial nerve palsy can be caused by a myriad of causes; in about two-thirds of the cases etiology is idiopathic or infective.8 Other causes include trauma, inflammatory and/or autoimmune diseases and primary or secondary tumors. Considering the sudden onset of facial paralysis and clinical presentation, our patient was initially diagnosed as an acute otitis with otogenic facial palsy. In absence of response to treatment (antibiotics, antiviral agents or steroids), CT scan is obligatory. Cases of prolonged facial paralysis are indicative of facial nerve exploration.9 During surgery of elderly patients with osteolytic temporal bone lesions, samples for histopathological analysis are obligatory; we found a soft, friable tissue prone to hemorrhage in the mastoid that was sent for histopathological analysis.
Chest radiographs are less sensitive and specific for lung cancer than CT scans; in our case, chest radiograph showed no sign of lung cancer. Histopathological and immunohistochemical analysis enabled accurate diagnosis with primary site identification. Further CT, bronchoscopic and histopathological examination confirmed the diagnosis of a primary lung adenocarcinoma. The whole diagnostic process lasted nearly three months, and our patient died without specific cancer treatment.
ConclusionMetastatic disease should always be considered in patients with facial nerve paralysis who also had a history of malignant disease. Our case is quite unique: otogenic facial palsy was an initial manifestation of lung cancer; the facial palsy was the result of temporal bone metastasis. Therefore, one should always exclude a possible temporal bone metastasis in elderly patients with and even without the history of malignant disease, especially when there is evidence of temporal bone osteolysis.4–7
Conflicts of interestThe authors declare no conflicts of interest.
This paper was supported, in part, by the Serbian Ministry of Science (Project No. 175026).
Please cite this article as: Djeric D, Boricic I, Tomanovic N, Cvorovic L, Blazic S, Folic M, et al. The facial palsy as first symptom of the temporal bone lung cancer metastasis. Braz J Otorhinolaryngol. 2017;83:720–2.
Peer Review under the responsibility of Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial.
gology is pleased to honor the reviewers


