
Tinnitus is a common disorder that occurs frequently across all strata of population and has an important health concern. Tinnitus is often associated with different forms of hearing loss of varying severity.
ObjectiveThe present study aimed to identify the association of tinnitus with hearing loss in various otological disorders of a South Indian population.
MethodsA total of 3255 subjects referred to the MAA ENT Hospital, Hyderabad, from 2004 to 2014, affected with various otological diseases have been included in the present cross-sectional study. Diagnosis of the diseases was confirmed by an ear, nose, and throat (ENT) specialist using detailed medical and clinical examination. Statistical analysis was performed using the χ2 test and binary logistic regression.
ResultsTinnitus was observed in 29.3% (956) of the total study subjects that showed an increased prevalence in greater than 40 years of age. There was a significant increase in risk of tinnitus with middle (OR=1.79, 95% CI=1.02–3.16) and inner (OR=3.00, 95% CI=1.65–5.45) inner ear diseases. It was noted that 96.9% (n=927) of the tinnitus subjects was associated with hearing loss. Otitis media (60.9%), presbycusis (16.6%) and otosclerosis (14.3%) are the very common otological disorders leading to tinnitus. Tinnitus was significantly associated with higher degree of hearing loss in chronic suppurative otitis media (CSOM) subjects.
ConclusionThe present study could identify the most prevalent otological risk factors leading to development of tinnitus with hearing loss in a South Indian population.
O zumbido é um distúrbio comum que ocorre com frequência em todos os estratos da população, constituindo um problema importante de saúde. O zumbido é frequentemente associado a diferentes formas de perda auditiva e sua gravidade é variada.
ObjetivoO presente estudo teve como objetivo identificar a associação entre zumbido e perda auditiva em várias doenças otológicas na população do Sul da Índia.
MétodoNo total, 3.255 indivíduos encaminhados ao Hospital MAA ENT em Hyderabad de 2004 a 2014, com diversas doenças otológicas, foram incluídos neste estudo transversal. O diagnóstico das doenças foi confirmado pelo otorrinolaringologista por meio de exames médico e clínico detalhados. A análise estatística foi realizada com o teste do χ2 e regressão logística binária.
ResultadosZumbido foi observado em 29,3% (956) do total de participantes do estudo, com maior prevalência em indivíduos com mais de 40 anos de idade. Houve um aumento significante do risco de zumbido em doenças da orelha média (OR=1,79, IC 95%=1,02-3,16) e interna (OR=3,00, IC 95%=1,65-5,45). Observamos que em 96,9% (n=927) dos indivíduos com zumbido houve associação com perda auditiva.
ConclusãoO presente estudo pôde identificar os fatores etiológicos mais prevalentes que levam ao desenvolvimento de zumbido associado à perda auditiva em uma população do Sul da Índia. Otite média (60,9%), presbiacusia (16,6%) e otosclerose (14,3%) são doenças otológicas frequentemente associadas ao zumbido. Em indivíduos com otite média crônica supurativa (OMCS), o zumbido foi significantemente associado ao maior grau de perda auditiva.
Tinnitus is a perceptional expression of any sound that originates in an involuntary manner, either unilaterally or bilaterally, in the absence of any external acoustic or electric stimulus.1,2 The etiology of tinnitus remains unknown, but some underlying clinical causes such as middle-ear diseases, nasal allergies, autoimmunity, cardiovascular diseases, diabetes, degenerative neural disorders, socio-demographic, and environmental factors have been reported.2–5 Many clinical studies have reported that otological disorders causes changes in the cochlear structures or neuroplastic alterations in the central auditory pathways, leading to tinnitus.2,4,6,7 Globally, about 10–15% of the general population is expected to be affected with tinnitus, with or without concomitant hearing impairment.4,8 Moreover, the prevalence of tinnitus correlates with the severity and frequency characteristics of the hearing loss.4,9 Further, tinnitus is present in 70–85% of hearing impairment caused by different pathologies of the auditory system.2,5,10 In India, it is estimated that approximately 4.5 million people are affected with tinnitus; unfortunately there are no exact data available on the prevalence and etiology of tinnitus.11 Therefore, the present study aimed to establish the prevalence and to identify the potential predisposing factors leading to tinnitus and hearing loss in a South Indian population.
MethodsSubjectsIn the present cross-sectional study, a total of 3255 patients with different otological diseases referred to MAA ENT Hospitals, Hyderabad, Telangana State, over a period of 10 years from 2004–2014 constituted the study subjects. All patients underwent a detailed medical examination and clinical history was recorded. Audiometric thresholds of hearing loss were evaluated using pure tone average for the frequencies 0.5, 1, 2, 4 and 8kHz. The study has been carried out with institutional ethics committee clearance.
Statistical analysisThe data obtained was coded for statistical evaluations. Appropriate statistical analysis was performed using PASW STATISTICS 18.0 (SPSS Inc. – Chicago, IL, United States). Continuous data is represented as means and standard deviations, whereas categorical data as proportions. The χ2 test was used to compare the proportions, while binary logistic regression analysis was performed for association of categorical variables.
ResultsAmong the 3255 study subjects with otological diseases, 58.6% (n=1906) were affected with ear-only diseases, 36.5% (n=1188) with nasal or nasopharyngeal and 4.9% (n=161) with metabolic disorders. Increase in prevalence of middle ear otological diseases i.e., 86.2% (n=2808), compared to inner ear 11.2% (n=364) and outer ear diseases 2.6% (n=83) was observed. The patients were aged between 7 and 83 years with a mean age of 36.0±18.94 with 58.4% (n=1902) males and 41.6% (n=1353) females. The prevalence of tinnitus was found to be 29.4% (n=956) among the study subjects.
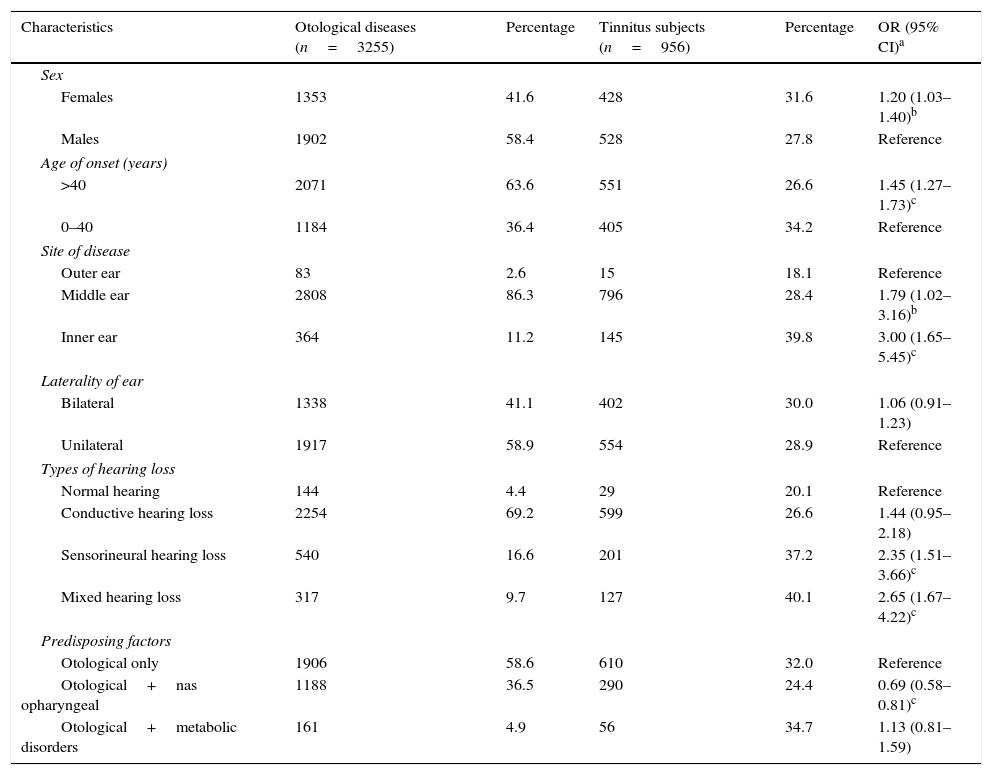
The percentage of tinnitus subjects affected with only ear ailments was 63.8% (n=610), nasal or nasopharyngeal was 30.3% (n=290), and metabolic disorders was 5.9% (n=56). The onset of tinnitus was at mean age of 32.2±20.45 and a significant increase in risk was seen in the age group >40 years (OR=1.45; 95% CI=1.27−1.73). Among the tinnitus subjects, 55.2% (n=528) were males and 44.8% (n=428) were females, with increased male preponderance of 1.23. However, significant increase in risk for females was observed (OR=1.20; 95% CI=1.03−1.40). The occurrence of tinnitus was found to be more of unilateral (58.0%) than bilateral (42.0%). However, no significant association was observed between tinnitus and laterality. The distribution of sex, age of onset, site of disease, laterality, type of hearing loss, and predisposing factors is represented in Table 1.
Clinical and demographic findings in subjects affected with tinnitus among otological disorders.
| Characteristics | Otological diseases (n=3255) | Percentage | Tinnitus subjects (n=956) | Percentage | OR (95% CI)a |
|---|---|---|---|---|---|
| Sex | |||||
| Females | 1353 | 41.6 | 428 | 31.6 | 1.20 (1.03–1.40)b |
| Males | 1902 | 58.4 | 528 | 27.8 | Reference |
| Age of onset (years) | |||||
| >40 | 2071 | 63.6 | 551 | 26.6 | 1.45 (1.27–1.73)c |
| 0–40 | 1184 | 36.4 | 405 | 34.2 | Reference |
| Site of disease | |||||
| Outer ear | 83 | 2.6 | 15 | 18.1 | Reference |
| Middle ear | 2808 | 86.3 | 796 | 28.4 | 1.79 (1.02–3.16)b |
| Inner ear | 364 | 11.2 | 145 | 39.8 | 3.00 (1.65–5.45)c |
| Laterality of ear | |||||
| Bilateral | 1338 | 41.1 | 402 | 30.0 | 1.06 (0.91–1.23) |
| Unilateral | 1917 | 58.9 | 554 | 28.9 | Reference |
| Types of hearing loss | |||||
| Normal hearing | 144 | 4.4 | 29 | 20.1 | Reference |
| Conductive hearing loss | 2254 | 69.2 | 599 | 26.6 | 1.44 (0.95–2.18) |
| Sensorineural hearing loss | 540 | 16.6 | 201 | 37.2 | 2.35 (1.51–3.66)c |
| Mixed hearing loss | 317 | 9.7 | 127 | 40.1 | 2.65 (1.67–4.22)c |
| Predisposing factors | |||||
| Otological only | 1906 | 58.6 | 610 | 32.0 | Reference |
| Otological+nas opharyngeal | 1188 | 36.5 | 290 | 24.4 | 0.69 (0.58–0.81)c |
| Otological+metabolic disorders | 161 | 4.9 | 56 | 34.7 | 1.13 (0.81–1.59) |
n, Frequency; 95% CI, 95% confidence interval; OR, odds ratio.
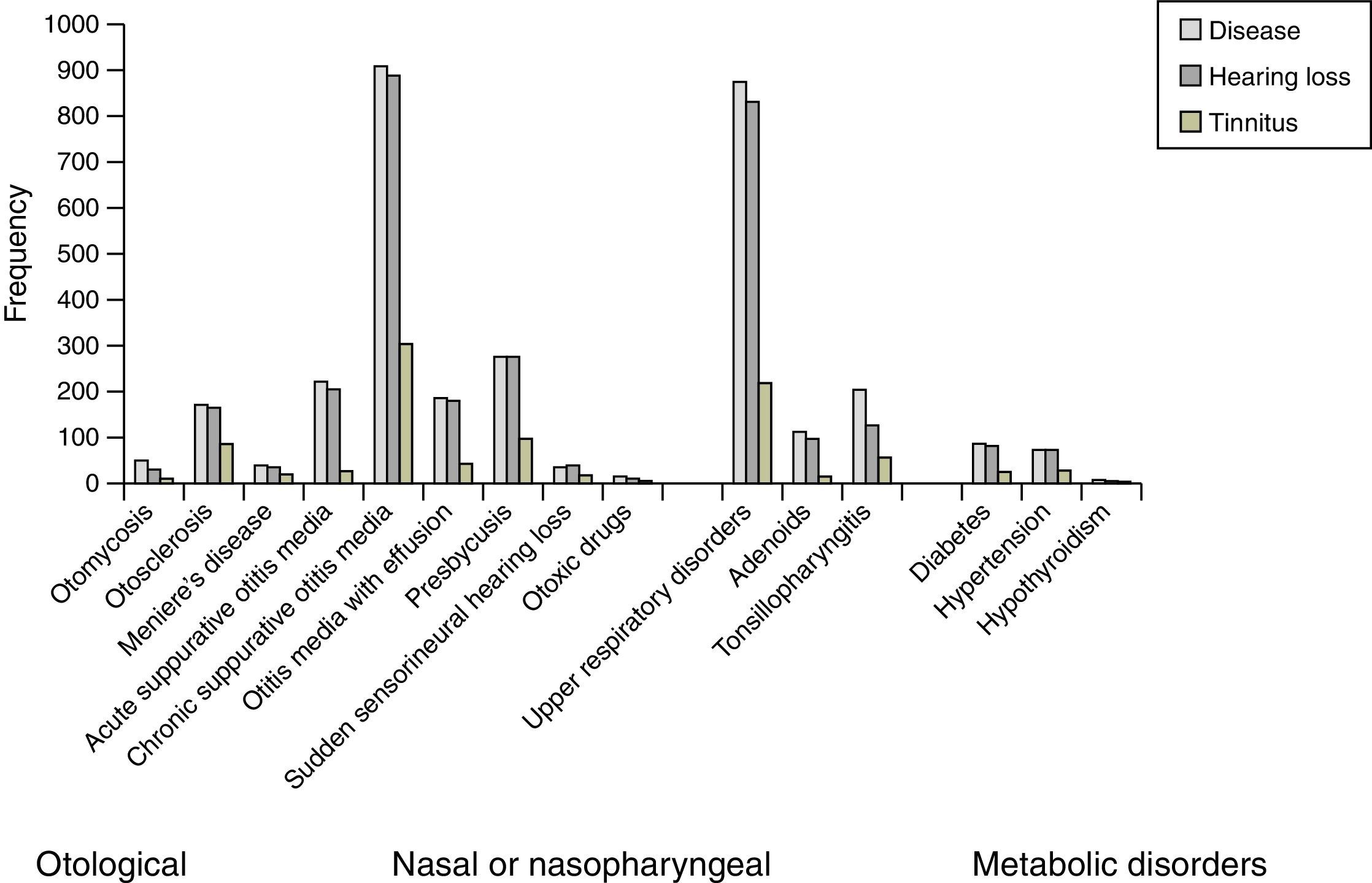
Risk of tinnitus was found to be significantly increased in subjects affected with inner ear 39.8% (OR=3.00; 95% CI=1.65−5.45), followed by middle ear diseases 28.4% (OR=1.79; 95% CI=1.02−3.16). Among the inner ear diseases, presbycusis (16.6%), Meniere's disease (3.3%), and sudden sensorineural hearing loss (SSNHL) (2.8%) were more prevalent. Chronic suppurative otitis media (CSOM) was found in 49.6%, otosclerosis in 14.2%, and otitis media with effusion (OME) in 7% of otological disorders, contributing to tinnitus in the middle ear. Among the other predisposing factors, upper respiratory disorders contributed to 69.4%, tonsillopharyngitis 10.6%, hypertension 2.9%, and diabetes 2.6% for tinnitus cases (Fig. 1).

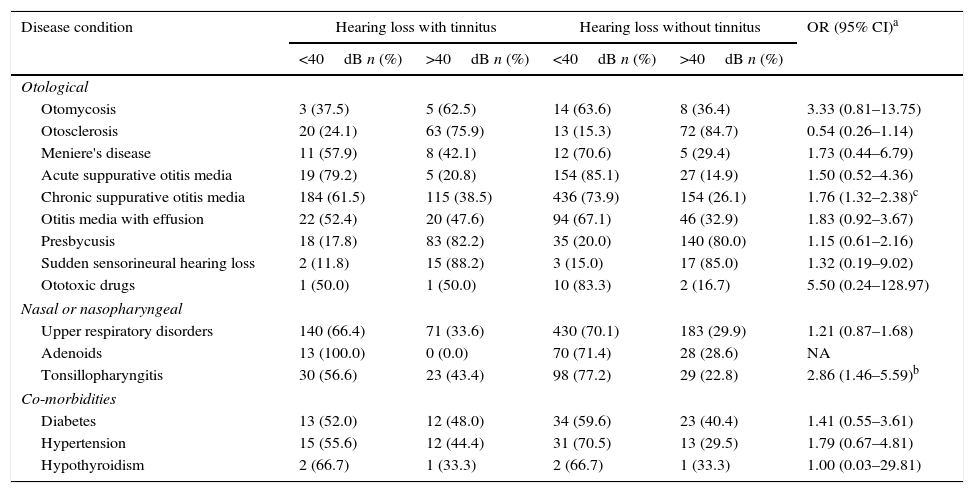
In the present study, the prevalence of hearing loss with tinnitus was 29.8% (n=927). The prevalence of various otological diseases predisposing to tinnitus is depicted in Fig. 1. The predisposing factors such as CSOM, OME, otomycosis, and Meniere's disease were associated with higher frequency (>40dB) of hearing loss in tinnitus subjects (Table 2). However, a significant association was noticed only in CSOM (OR=1.76; 95% CI=1.32−2.38). Further it is also observed that other predisposing factors were also associated at higher frequency of hearing loss. Among them, tonsillopharyngitis showed statistical significance (OR=2.86; 95% CI=1.46−5.59) (Table 2).
Degree of hearing loss in subjects with and without tinnitus in otological disorders.
| Disease condition | Hearing loss with tinnitus | Hearing loss without tinnitus | OR (95% CI)a | ||
|---|---|---|---|---|---|
| <40dB n (%) | >40dB n (%) | <40dB n (%) | >40dB n (%) | ||
| Otological | |||||
| Otomycosis | 3 (37.5) | 5 (62.5) | 14 (63.6) | 8 (36.4) | 3.33 (0.81–13.75) |
| Otosclerosis | 20 (24.1) | 63 (75.9) | 13 (15.3) | 72 (84.7) | 0.54 (0.26–1.14) |
| Meniere's disease | 11 (57.9) | 8 (42.1) | 12 (70.6) | 5 (29.4) | 1.73 (0.44–6.79) |
| Acute suppurative otitis media | 19 (79.2) | 5 (20.8) | 154 (85.1) | 27 (14.9) | 1.50 (0.52–4.36) |
| Chronic suppurative otitis media | 184 (61.5) | 115 (38.5) | 436 (73.9) | 154 (26.1) | 1.76 (1.32–2.38)c |
| Otitis media with effusion | 22 (52.4) | 20 (47.6) | 94 (67.1) | 46 (32.9) | 1.83 (0.92–3.67) |
| Presbycusis | 18 (17.8) | 83 (82.2) | 35 (20.0) | 140 (80.0) | 1.15 (0.61–2.16) |
| Sudden sensorineural hearing loss | 2 (11.8) | 15 (88.2) | 3 (15.0) | 17 (85.0) | 1.32 (0.19–9.02) |
| Ototoxic drugs | 1 (50.0) | 1 (50.0) | 10 (83.3) | 2 (16.7) | 5.50 (0.24–128.97) |
| Nasal or nasopharyngeal | |||||
| Upper respiratory disorders | 140 (66.4) | 71 (33.6) | 430 (70.1) | 183 (29.9) | 1.21 (0.87–1.68) |
| Adenoids | 13 (100.0) | 0 (0.0) | 70 (71.4) | 28 (28.6) | NA |
| Tonsillopharyngitis | 30 (56.6) | 23 (43.4) | 98 (77.2) | 29 (22.8) | 2.86 (1.46–5.59)b |
| Co-morbidities | |||||
| Diabetes | 13 (52.0) | 12 (48.0) | 34 (59.6) | 23 (40.4) | 1.41 (0.55–3.61) |
| Hypertension | 15 (55.6) | 12 (44.4) | 31 (70.5) | 13 (29.5) | 1.79 (0.67–4.81) |
| Hypothyroidism | 2 (66.7) | 1 (33.3) | 2 (66.7) | 1 (33.3) | 1.00 (0.03–29.81) |
n, Frequency; OR, odds ratio; 95% CI, 95% confidence interval; NA, not applicable.
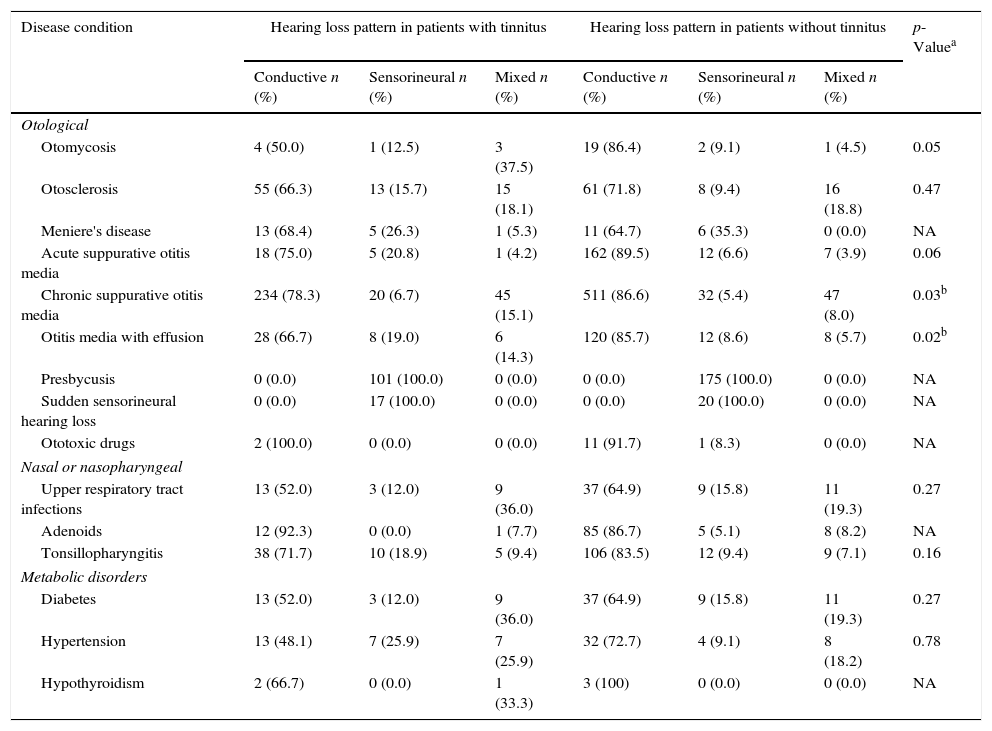
With regard to pattern of hearing loss, conductive type was observed in 62.6% (n=599), sensorineural in 21.0% (n=201) and mixed type in 13.3% (n=127) of tinnitus cases (Table 3). It was observed that there is a significant association of tinnitus with sensorineural (37.2%) and mixed hearing loss (40.1%) when compared to conductive hearing loss (26.6%) (Table 1, Fig. 1). High prevalence of sensorineural and mixed hearing loss was observed in tinnitus cases affected with otitis media (Table 3).
Pattern of hearing loss in subjects with and without tinnitus in otological disorders.
| Disease condition | Hearing loss pattern in patients with tinnitus | Hearing loss pattern in patients without tinnitus | p-Valuea | ||||
|---|---|---|---|---|---|---|---|
| Conductive n (%) | Sensorineural n (%) | Mixed n (%) | Conductive n (%) | Sensorineural n (%) | Mixed n (%) | ||
| Otological | |||||||
| Otomycosis | 4 (50.0) | 1 (12.5) | 3 (37.5) | 19 (86.4) | 2 (9.1) | 1 (4.5) | 0.05 |
| Otosclerosis | 55 (66.3) | 13 (15.7) | 15 (18.1) | 61 (71.8) | 8 (9.4) | 16 (18.8) | 0.47 |
| Meniere's disease | 13 (68.4) | 5 (26.3) | 1 (5.3) | 11 (64.7) | 6 (35.3) | 0 (0.0) | NA |
| Acute suppurative otitis media | 18 (75.0) | 5 (20.8) | 1 (4.2) | 162 (89.5) | 12 (6.6) | 7 (3.9) | 0.06 |
| Chronic suppurative otitis media | 234 (78.3) | 20 (6.7) | 45 (15.1) | 511 (86.6) | 32 (5.4) | 47 (8.0) | 0.03b |
| Otitis media with effusion | 28 (66.7) | 8 (19.0) | 6 (14.3) | 120 (85.7) | 12 (8.6) | 8 (5.7) | 0.02b |
| Presbycusis | 0 (0.0) | 101 (100.0) | 0 (0.0) | 0 (0.0) | 175 (100.0) | 0 (0.0) | NA |
| Sudden sensorineural hearing loss | 0 (0.0) | 17 (100.0) | 0 (0.0) | 0 (0.0) | 20 (100.0) | 0 (0.0) | NA |
| Ototoxic drugs | 2 (100.0) | 0 (0.0) | 0 (0.0) | 11 (91.7) | 1 (8.3) | 0 (0.0) | NA |
| Nasal or nasopharyngeal | |||||||
| Upper respiratory tract infections | 13 (52.0) | 3 (12.0) | 9 (36.0) | 37 (64.9) | 9 (15.8) | 11 (19.3) | 0.27 |
| Adenoids | 12 (92.3) | 0 (0.0) | 1 (7.7) | 85 (86.7) | 5 (5.1) | 8 (8.2) | NA |
| Tonsillopharyngitis | 38 (71.7) | 10 (18.9) | 5 (9.4) | 106 (83.5) | 12 (9.4) | 9 (7.1) | 0.16 |
| Metabolic disorders | |||||||
| Diabetes | 13 (52.0) | 3 (12.0) | 9 (36.0) | 37 (64.9) | 9 (15.8) | 11 (19.3) | 0.27 |
| Hypertension | 13 (48.1) | 7 (25.9) | 7 (25.9) | 32 (72.7) | 4 (9.1) | 8 (18.2) | 0.78 |
| Hypothyroidism | 2 (66.7) | 0 (0.0) | 1 (33.3) | 3 (100) | 0 (0.0) | 0 (0.0) | NA |
n, Frequency; NA, not applicable.
Tinnitus is a common disorder which occurs frequently across all strata of population and exhibits an important health concern. Clinical and epidemiological studies on tinnitus have revealed that 5–32% of the world population is affected with tinnitus.2,12,13 Many risk factors associated with onset of tinnitus have been reported, of which the most prominent are age, gender, auditory, metabolic and neurological disorders, vascular alterations, dental factors, exposure to noise, ototoxic drugs, caffeine, nicotine, and alcohol.4,8,9,14 Otological disorders are the most common cause of tinnitus.15 Various otological diseases can lead to tinnitus and different types of hearing loss. This is due to infection or stiffening of bones or spasms of one of the two tiny muscles attached to bones of the middle ear, which affects the sound transmission system in the ear.9,16,17 Furthermore, various nasopharyngeal factors are involved in Eustachian tube dysfunction, predisposing to middle ear infections. In the present study, 29.3% of the otological disorders were affected with tinnitus, of which 30.3% were affected with nasal or nasopharyngeal factors especially tonsillopharyngitis in particular causing Eustachian tube dysfunction and middle ear infection leading to hearing loss and tinnitus, probably through lymphatic spread. However this needs to be further studied.
Many studies conducted on tinnitus have reported high male preponderance, which was mainly attributed to high environmental and occupational exposure.2,18,19 However, higher female preponderance of tinnitus has also been reported by a few studies.20 In the present study, tinnitus has been found to affect both males and females, but with a high male preponderance, which is due to the greater number of male subjects visiting the hospital when compared to females. However, it was also noticed that there was a significant increase in female cases for the treatment at the chronic stage of ear diseases/tinnitus.
The onset of tinnitus is reported to have a strong association with increasing age but it was also found to be present in younger age.5,6,16,21 Differences in the onset of tinnitus are due to ethnicity, age variation, and the diagnostic criteria that have been taken into consideration.5,22,23 In the present study, higher prevalence of tinnitus has been discovered in the age group greater than 40 years. Changes in life style, abnormality at the metabolic level, and a high incidence of predisposing factors of metabolic diseases experienced by the elderly people are reported to cause tinnitus. Moreover, increased level of insulin resistance and some drugs used for the treatment of hypertension worsen the resistance and can favor tinnitus onset.21,24 In the present study, tinnitus was observed in 30.1% of patients with diabetes mellitus, 38.8% in hypertension and 40% with hypothyroidism. Medications such as salicylates, aminoglycoside antibiotics, quinine, or cisplatin used to treat otological and nasopharyngeal diseases can cause damage to the cochlea and trigger or enhance tinnitus.1,25,26 It was found that 13.3% of ototoxicity cases contributed to tinnitus in the present study.
Hearing loss and tinnitus are closely related, as the prevalence of hearing loss is higher in tinnitus cases.5,24 In the present study, 96.9% of cases with tinnitus have a significant association with hearing loss, indicating it as one of the crucial risk factors. Moreover, the occurrence of hearing loss at higher frequencies in tinnitus subjects indicates the severity of suffering caused due to otological disorders.27,28 Further, auditory pathology in middle and inner parts of ear can lead to different pattern of hearing loss. Interestingly, in the present study it was observed that conductive form is the most common cause of hearing loss and tinnitus when compared to sensorineural hearing loss. In addition, middle ear diseases in this study were more compromised than the inner ear, unlike other studies.29,30 This variation could be attributed to geographical distribution and socioeconomic status. Further, in the present study 95% of middle ear diseases obtained relief from hearing loss and 86% from tinnitus after treatment with surgical and medical interventions. In the present study, there was a significant increase in hearing loss at higher frequency with sensorineural and mixed type in tinnitus subjects with CSOM. The results indicate CSOM as one of the most common otological diseases affecting the middle and inner ear leading to tinnitus and hearing loss.
In conclusion, the present study indicates otitis media, presbycusis, and otosclerosis are the most common contributing factors leading to tinnitus and hearing loss. The prevalence of tinnitus increased with the progression of the otological disorders. Hence, efforts to control these risk factors may help in ameliorating tinnitus and improving quality of life of the affected individuals. Further studies on the genetics of tinnitus associated with hearing loss will undoubtedly lead to effective therapeutic approaches and clinical management of tinnitus.
Conflicts of interestThe authors declare no conflicts of interests.
The authors thank Mrs. B. Sunita G Kumar, CMD, MAA ENT Hospitals for her support and cooperation in carrying out the work. We also thank Dr. Balakrishna of NIN for providing support in performing the statistical analysis.
Please cite this article as: Manche SK, Madhavi J, Meganadh KR, Jyothy A. Association of tinnitus and hearing loss in otological disorders: a decade-long epidemiological study in a South Indian population. Braz J Otorhinolaryngol. 2016;82:643–9.


