


Rhabdomyomas are benign mesenchymal tumors composed of striated mature skeletal muscle cells, being no more than 2% of all striated muscle tumors,1 distinguished in cardiac and extracardiac subtypes. Cardiac rhabdomyomas occur generally in children and are considered hamartomatous lesions, often associated with phacomatoses, such as tuberous sclerosis,1,2 and hamartomas of the kidney and other organs.1 Extracardiac rhabdomyomas are clinically and morphologically subdivided in three subtypes: the vaginal, fetal and adult variants. The vaginal-type is a rare tumor-like polypoid mass, found in the vagina and vulva of middle-aged women. The fetal-type, with the subordinated juvenile rhabdomyoma,3 is prevalent in head and neck areas in children. Adult extracardiac rhabdomyomas present generally as unifocal head and neck tumors in middle-aged patients,4,5 multifocal in 14–26% of cases.6 Adult rhabdomyomas occur in the soft tissues of the head and neck up to 70–93% of cases,1 while glottic lesions are extremely rare, and only 22 cases have been reported up to now. With this article we report an additional case of glottic adult-type rhabdomyoma and review the pertinent literature, with two aims: (I) assess the standard of care of this pathology, to avoid inadequate treatment and (II) increase its knowledge among surgeons and pathologists.
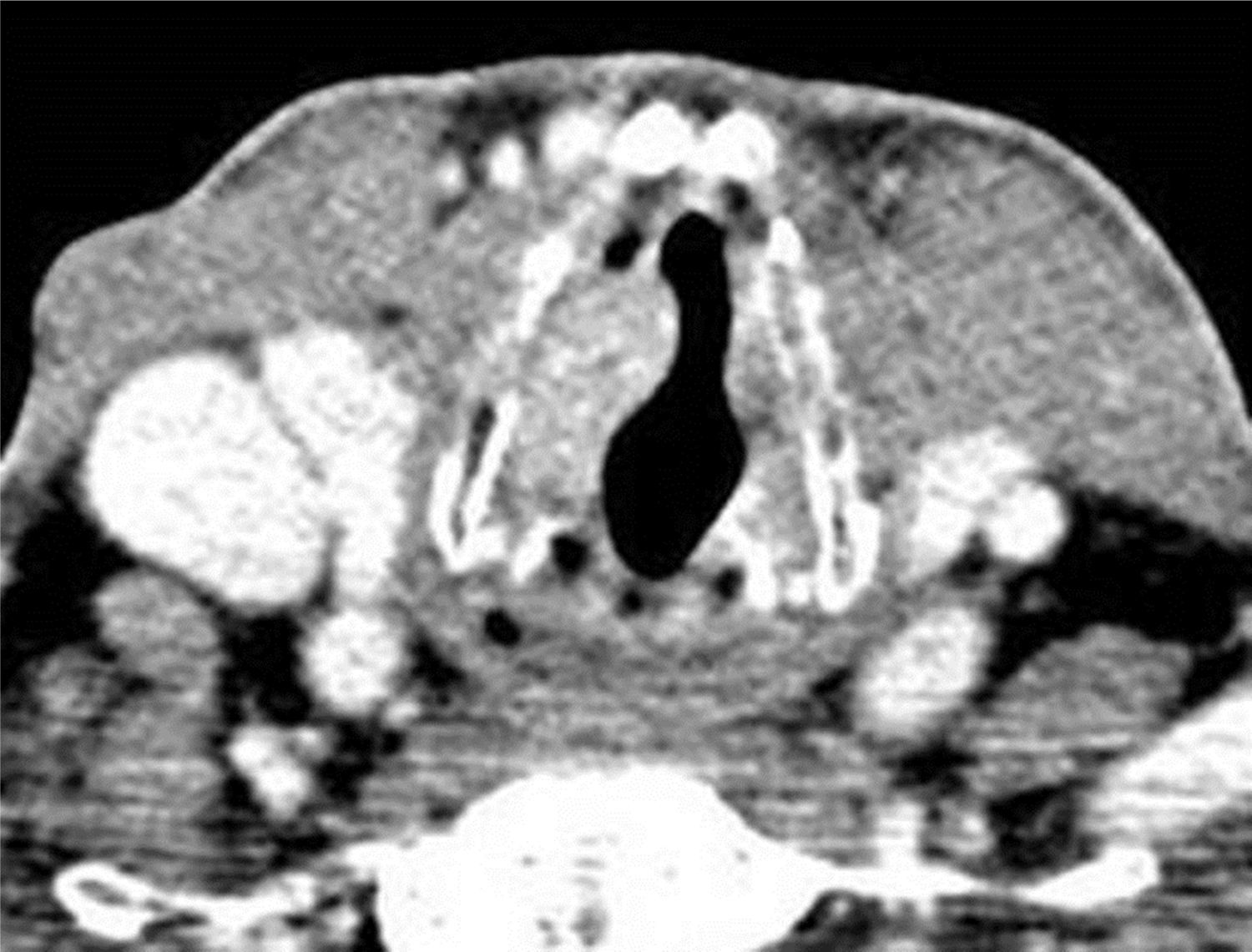
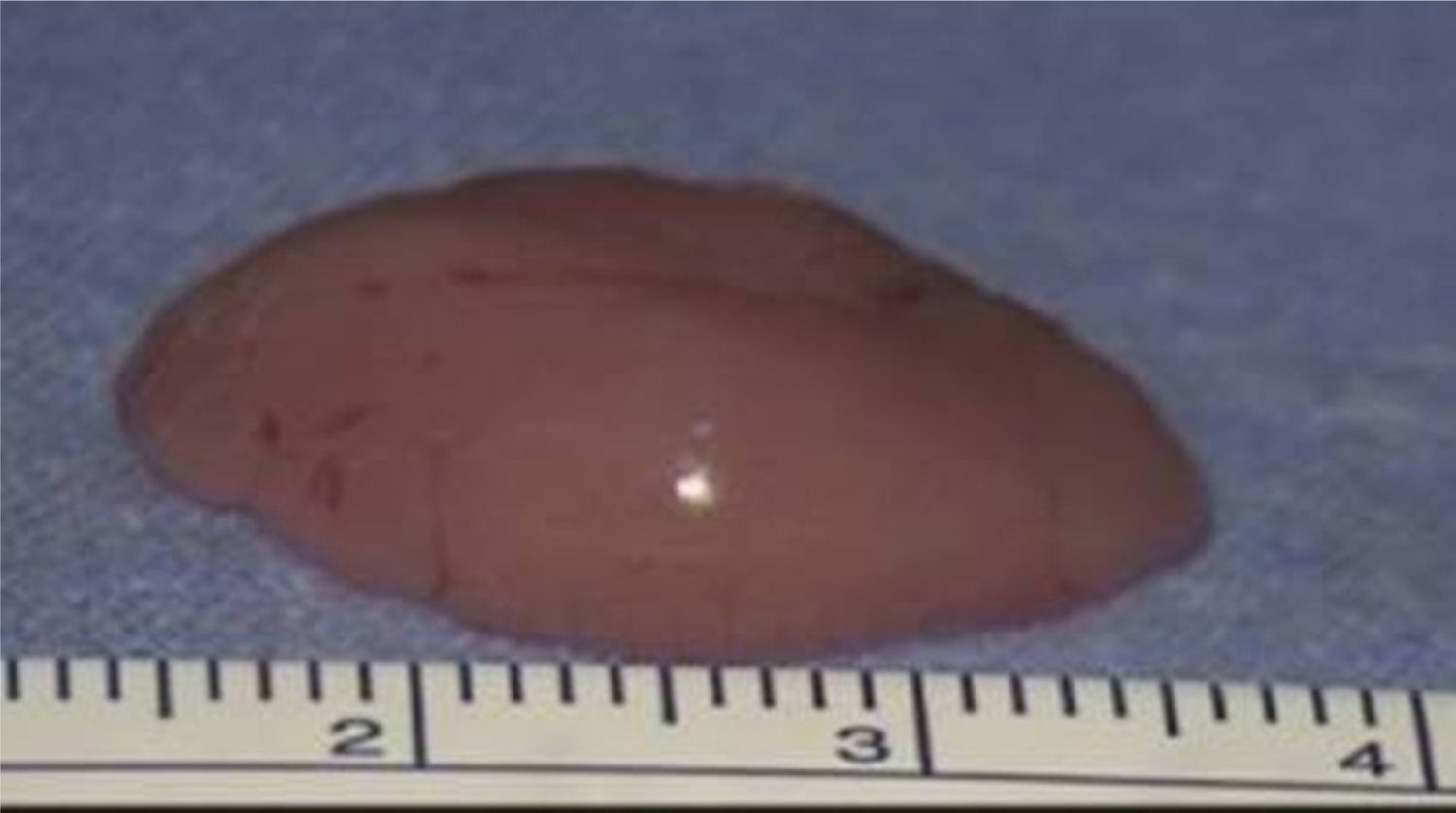
Case reportA 75-year-old male was referred to our department with a 4-year history of progressive dysphonia. Flexible scope examination showed a smooth submucosal swelling of the middle third of the right vocal cord, associated with impairment of vocal cord mobility. Contrast-enhanced computed tomography (CT) of the neck showed a deep right vocal cord lesion extended to the anterior paraglottic space, with low and uniform pathologic enhancement (Fig. 1). Clinical and radiological features suggested its benign nature and, therefore, conservative surgery was planned. The patient underwent transoral CO2 laser excision under general anesthesia with CO2 laser (Digital AcuBlade™, Lumenis™, Israel) set on 10 Watts, continuous wave in Super-Pulsed mode/emission, Acu-Blade 2mm of length, under microscopic vision (focal length of 400mm), through a microflap technique leaving the mucosa of the vocal cord intact. The tumor, deeply situated into the right vocal cord, was easily “en bloc” enucleated and appeared as an oval nodule of 22mm in greatest dimension (Fig. 2). After the excision, the minus into the right thyro aritenoid muscle (Fig. 3) was left to heal by secondary intention. Postoperative course was uneventful: the patient was discharged 1 day after surgery and he regained normal vocal cord mobility and normal voice within 4 weeks. At histology, typical morphologic features of adult rhabdomyoma with sheets of large polygonal cells separated by few connective tissues were present. The cells had abundant eosinophilic cytoplasm with eccentrically placed nuclei, whereas in some areas cytoplasmic vacuolization with a centrally placed nucleus was found. Immunohistochemistry showed the cells to be strongly positive to skeletric muscle actin and desmin. At 12-month follow-up, the complete closure of the minus was observed (Fig. 4), with no evidence of recurrence.




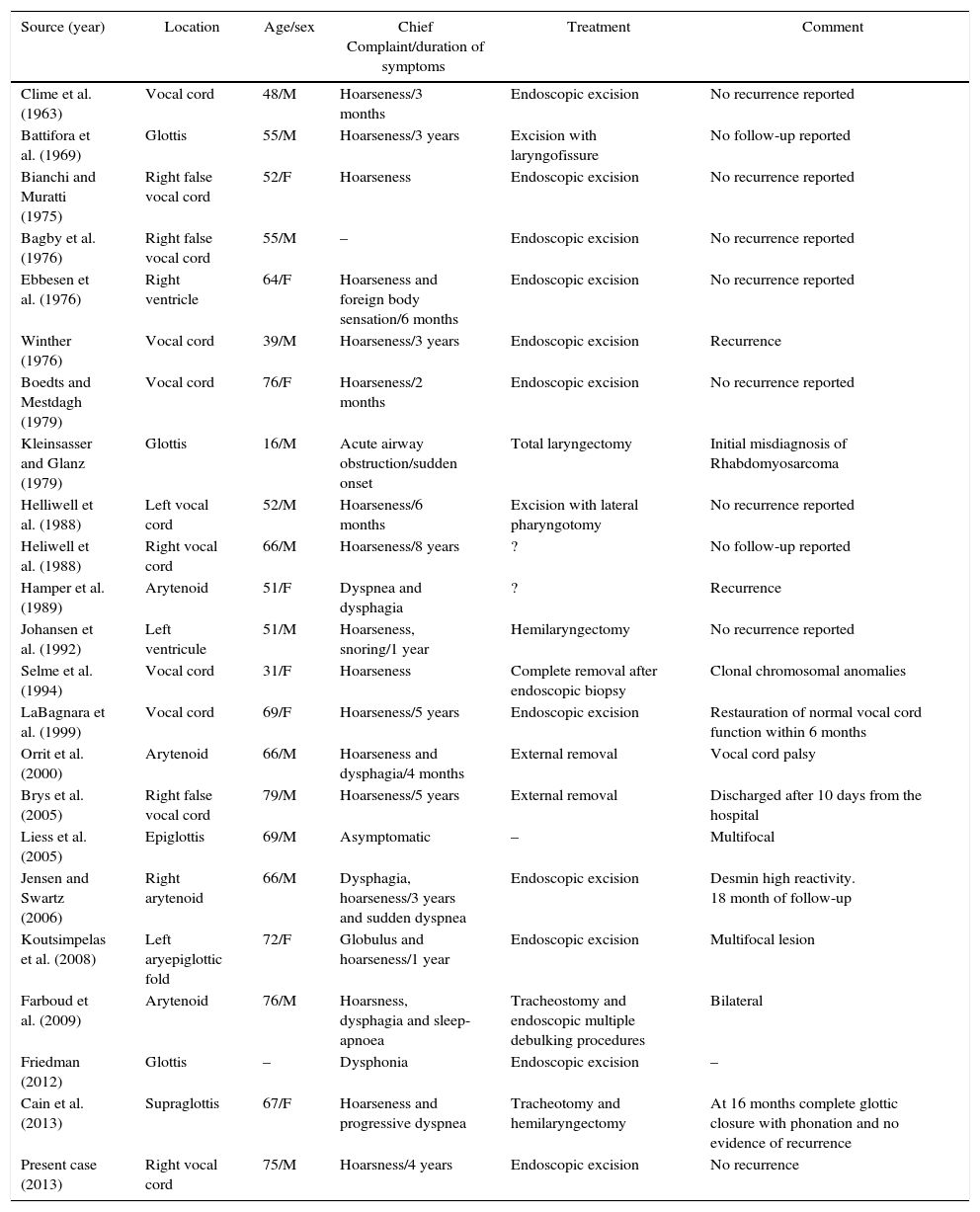
Extracardiac adult and fetal types rhabdomyomas probably originate from skeletal muscle of the third and fourth branchial arches.1,7 Their neoplastic nature was not clear because tumor cells usually do not express cell proliferation markers such as Ki-67 and PCNA, resembling more likely hamartomas than neoplasms.7 In 1992, Gibas and Miettinem demonstrated few chromosomal clonal anomalies supporting the neoplastic nature of rhabdomyomas.8 Before this case, 22 cases of adult-type laryngeal rhabdomyomas have been reported (Table 1): Johansen and coworkers, in 1995, reviewed all cases of adult rhabdomyomas of the larynx (n=12) previously described1; after 1995, 10 further cases have been published. Age ranges from 16-year old to 79-year old (mean age 59 years, 59% of patients in the sixth and seventh decades, sex ratio M/F of 1:1.75); the tumor was found in the glottis in 12 cases, in the arytenoid in 4 patients and in the supraglottis in 7 patients; although stridor and airway obstruction can develop abruptly, the lesion generally remains asymptomatic, until it causes symptoms like dysphonia (86%), dysphagia (18%) and dyspnea (18%), that usually progress slowly (median duration-time of 2.5 years) (Table 1). Macroscopic appearance is usually a submucosal swelling with possible deep extension inside the laryngeal framework, but they may be sessile. Differential diagnoses include neurogenic or vascular tumors, oncocytoma, osteoma, Abrikossoff's tumor and rhabdomyomasarcoma.1 Radiographically adult rhabdomyoma presents as an homogenous lesion, isointense or slightly hyperintense to muscle on T1- as well as T2-weighted MRI and slightly hyperdense on CT.4 At histology, the adult and the fetal type have to be distinguished: the former closely mimics the structure of adult skeletal muscle and contains cells with PAS-positive granular or vacuolated cytoplasm, while the fetal type is composed with less differentiated neoplastic cells.3 Immunohistochemistry demonstrates the muscle immunophenotype, with strong positivity for muscle specific markers; in our case and in the literature, desmin appeared as a reliable marker.1,2
Adult-type laryngeal rhabdomyomas.
| Source (year) | Location | Age/sex | Chief Complaint/duration of symptoms | Treatment | Comment |
|---|---|---|---|---|---|
| Clime et al. (1963) | Vocal cord | 48/M | Hoarseness/3 months | Endoscopic excision | No recurrence reported |
| Battifora et al. (1969) | Glottis | 55/M | Hoarseness/3 years | Excision with laryngofissure | No follow-up reported |
| Bianchi and Muratti (1975) | Right false vocal cord | 52/F | Hoarseness | Endoscopic excision | No recurrence reported |
| Bagby et al. (1976) | Right false vocal cord | 55/M | – | Endoscopic excision | No recurrence reported |
| Ebbesen et al. (1976) | Right ventricle | 64/F | Hoarseness and foreign body sensation/6 months | Endoscopic excision | No recurrence reported |
| Winther (1976) | Vocal cord | 39/M | Hoarseness/3 years | Endoscopic excision | Recurrence |
| Boedts and Mestdagh (1979) | Vocal cord | 76/F | Hoarseness/2 months | Endoscopic excision | No recurrence reported |
| Kleinsasser and Glanz (1979) | Glottis | 16/M | Acute airway obstruction/sudden onset | Total laryngectomy | Initial misdiagnosis of Rhabdomyosarcoma |
| Helliwell et al. (1988) | Left vocal cord | 52/M | Hoarseness/6 months | Excision with lateral pharyngotomy | No recurrence reported |
| Heliwell et al. (1988) | Right vocal cord | 66/M | Hoarseness/8 years | ? | No follow-up reported |
| Hamper et al. (1989) | Arytenoid | 51/F | Dyspnea and dysphagia | ? | Recurrence |
| Johansen et al. (1992) | Left ventricule | 51/M | Hoarseness, snoring/1 year | Hemilaryngectomy | No recurrence reported |
| Selme et al. (1994) | Vocal cord | 31/F | Hoarseness | Complete removal after endoscopic biopsy | Clonal chromosomal anomalies |
| LaBagnara et al. (1999) | Vocal cord | 69/F | Hoarseness/5 years | Endoscopic excision | Restauration of normal vocal cord function within 6 months |
| Orrit et al. (2000) | Arytenoid | 66/M | Hoarseness and dysphagia/4 months | External removal | Vocal cord palsy |
| Brys et al. (2005) | Right false vocal cord | 79/M | Hoarseness/5 years | External removal | Discharged after 10 days from the hospital |
| Liess et al. (2005) | Epiglottis | 69/M | Asymptomatic | – | Multifocal |
| Jensen and Swartz (2006) | Right arytenoid | 66/M | Dysphagia, hoarseness/3 years and sudden dyspnea | Endoscopic excision | Desmin high reactivity. 18 month of follow-up |
| Koutsimpelas et al. (2008) | Left aryepiglottic fold | 72/F | Globulus and hoarseness/1 year | Endoscopic excision | Multifocal lesion |
| Farboud et al. (2009) | Arytenoid | 76/M | Hoarsness, dysphagia and sleep-apnoea | Tracheostomy and endoscopic multiple debulking procedures | Bilateral |
| Friedman (2012) | Glottis | – | Dysphonia | Endoscopic excision | – |
| Cain et al. (2013) | Supraglottis | 67/F | Hoarseness and progressive dyspnea | Tracheotomy and hemilaryngectomy | At 16 months complete glottic closure with phonation and no evidence of recurrence |
| Present case (2013) | Right vocal cord | 75/M | Hoarsness/4 years | Endoscopic excision | No recurrence |
Definitive treatment for laryngeal adult rhabdomyoma is complete excision; although extensive lesions reported in the literature required in 8 cases an external approach (Table 1), including a total laryngectomy, when glottic rhabdomyoma is confined to the endolarynx, the transoral approach should be preferred. Transoral minimally invasive laser CO2 assisted excision appears to be optimal in terms of efficacy and low morbidity: the vocalis muscle and the mucosa can be only incised without any removal. Since dedifferentiation of an adult rhabdomyoma to a malignant variety is not documented, a more invasive approach may appear an overtreatment, but a radical excision is mandatory since recurrences are possible (2 cases in the literature),9,10 attributable to incomplete primary excision, that can occur since the consistence of the lesion is friable.
ConclusionLaryngeal rhabdomyoma is a rare benign tumor that has to be considered in the differential diagnosis of all submucosal laryngeal lesions. Conservative approach is advisable since the tumor can be endoscopically enucleated.
Conflicts of interestThe authors declare no conflicts of interest.
The authors gratefully acknowledge Sardinia Regional Government for the financial support (P.O.R. Sardegna F.S.E. Operational Programme of the Autonomous Region of Sardinia, European Social Fund 2007–2013 – Axis IV Human Resources, Objective l.3, Line of Activity l.3.1 “Avviso di chiamata per il finanziamento di Assegni di Ricerca”).
Please cite this article as: Carta F, Sionis S, Gerosa C, Puxeddu R. Endoscopic management of adult-type rhabdomyoma of the glottis: case report and review of the literature. Braz J Otorhinolaryngol. 2016;82:244–7.


