

Intrathyroid metastases represent one to three percent of thyroid cancers1–3; however, intrathyroid chondrosarcoma metastases are very rare indeed, as there are, to our knowledge, only four other cases reported in the literature.4–6 This case stands out, as the thyroid mass appeared 14 years after the treatment of the initial chondrosarcoma, without any other local of distant recurrence.
Case reportA male patient of Moroccan descent, 62 years of age, came to our department in 2014 for a large mass centered on the right thyroid lobe. Medical history included high blood pressure, obesity and type 2 diabetes, with severe chronic kidney failure. He had also been operated successfully 14 years ago in our hospital for a chondrosarcoma of the right femur. A close clinical, yearly follow-up had, to date, shown no local or distant recurrence, and the patient had no functional deficit. At the time, the patient had consulted in the orthopedic department of our hospital for pain in the upper leg, which had been increasing for over a year. A biopsy in January 2000 diagnosed a chondrosarcoma. The patient was operated two months later, and a large excision of the femur and the surrounding muscles (including the biopsy needle path) was performed. The tumor measured 60mm×40mm and was centered on the great trochanter and femur neck. The analysis found a grade II chondrosarcoma with cortical bone lysis (Fig. 1), with wide resection margins. There was no further radiotherapy or chemotherapy.
 and thyroid metastasis 14 years later (left and center). Both lesions were confirmed to be identical by a laboratory specialized in sarcoma (Oscar Lambret in Lille, France). Left: thyroid metastasis, HES staining ×2.5; myxoid tumor infiltrating the thyroid tissue and dissociating thyroid vesicles. Center: vascular invasion in the thyroid metastasis; HES staining ×10; cluster of dedifferentiated chondrocytes in a myxoid stroma, covered by an endothelial layer in a vessel lumen. Right: femur chondrosarcoma, HES staining ×2.5; showing massive bone resorption by a myxoid and chondroid tumor.")
Comparison of histology of the initial chondrosarcoma (right) and thyroid metastasis 14 years later (left and center). Both lesions were confirmed to be identical by a laboratory specialized in sarcoma (Oscar Lambret in Lille, France). Left: thyroid metastasis, HES staining ×2.5; myxoid tumor infiltrating the thyroid tissue and dissociating thyroid vesicles. Center: vascular invasion in the thyroid metastasis; HES staining ×10; cluster of dedifferentiated chondrocytes in a myxoid stroma, covered by an endothelial layer in a vessel lumen. Right: femur chondrosarcoma, HES staining ×2.5; showing massive bone resorption by a myxoid and chondroid tumor.
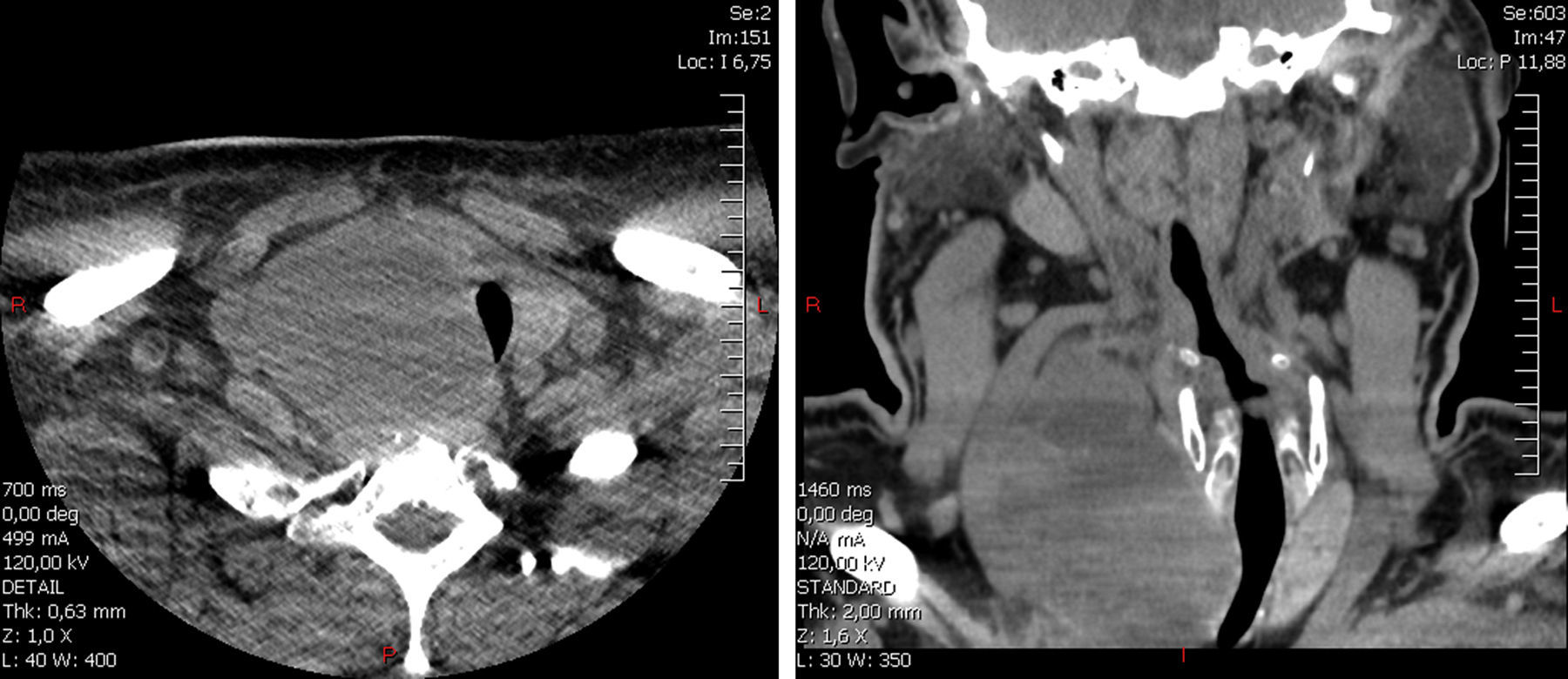
The patient came to our department in June 2014 for a thyroid mass which had been growing over the past few months and was becoming compressive. The patient presented mild dysphagia and dyspnea. The endoscopic examination revealed a deviated trachea, but good vocal cord function. The CT-scan (Fig. 2) showed a large mass in the right thyroid lobe with an important tracheal deviation, without any adenopathy. An ultrasound found a heterogenic mass measuring 90mm×54mm×68mm US guided fine-needle aspiration was not conclusive (very few cells). Thyroid blood tests were normal (TSH, T3, T4 and antibodies), and the patient did not present any hormonal disorders.
 and important tracheal and vessel deviation on the coronal plane (right). The mass measured 90mm×54mm×68mm.")
CT-scan of the thyroid mass. Due to the patient's chronic kidney failure, intravenous contrast could not be used. Note the important tracheal compression on the transverse plane (left) and important tracheal and vessel deviation on the coronal plane (right). The mass measured 90mm×54mm×68mm.
Due to the compressive symptoms and lack of diagnosis, a total thyroidectomy was performed three months later. Other than the size, the main operative difficulty was separating the mass from the carotid artery, to which it was very adherent. Additionally, a cystic mass in the right lobe was open laterally, and the muscles covering it had to be included in the resection. The right recurrent nerve was located in inflammatory tissue in between the mass and the trachea and was difficult to dissect. Perioperative frozen sections were non-conclusive. The patient was discharged after five days, and the immediate follow-up showed partial right recurrent nerve palsy without any functional consequence.
Analysis of the mass in our hospital showed a cystic myxoid tumor measuring over 40mm, identical to the femur lesion treated 14 years earlier. It also showed vascular invasion and infiltration of the lateral aspect of the right thyroid lobe. A probable chondrosarcoma metastasis was diagnosed (Fig. 1). The histology slides of thyroid and femur lesions were sent to a sarcoma reference center (Center Oscar Lambret, Lille, France), and the diagnosis was confirmed.
The case was then discussed in a sarcoma specialized board. No further treatment was decided regarding the thyroid metastasis, as the surgical excision was deemed complete. However, a second metastasis (10cm) in the right lung was discovered, prompting further pulmonary surgery (lobectomy). In the following months, a second pulmonary metastasis and an inoperable cervical recurrence were discovered. The patient died three months later after palliative chemotherapy.
DiscussionIntrathyroid metastases represent 1.4 to three percent of all thyroid cancers2; however, systematic post-mortem examinations have revealed that asymptomatic thyroid metastasis are much more common, in up to 24 percent of cases.2 Studies show that intrathyroid metastases are mostly due to kidney or otherwise lung and breast cancer.1–3 In most cases, the thyroid metastases are associated with multifocal metastases, with a very low survival rate. Thyroidectomy is usually performed to prevent local complications (compressive or invasive) and to help diagnose the primary cancer.1–3 As in this case, metastases to the thyroid are known to sometimes occur decades after the primary cancer.1–4 We have only found in the literature three cases of chondrosarcoma metastasizing to the thyroid, emphasizing how rare this condition is. In all cases, the patients rapidly died of multiple metastases.4,5
Chondrosarcoma has a high level of local recurrence, and the common treatment is surgery with a large en bloc excision, as they are usually resistant to radiotherapy and chemotherapy.7,8 Follow-up must be over a long period, as metastases are known to appear over a decade after the primary lesion.7–10 Although grade III lesions often have metastasis, grade I never do, and grade II only do in 10 percent of cases; therefore, low grade tumors have an excellent survival rate after large resection.9
Treatment of chondrosarcomas in the head and neck differs, as they are usually low grade with a low risk of metastasis.9,10 Furthermore, like in this case, as complete resection with margins is rarely possible (especially in the skull base), adjuvant radiotherapy is often performed after surgery.7,10
In this case, adjuvant radiotherapy was considered due to the muscle invasion and adherence to the carotid artery and the absence of resection of the fine-needle aspiration path, which is usually performed in chondrosarcoma. In fact, the cervical surgery was deemed sufficient, and the priority was shifted to the lung. Retrospectively, a more aggressive stance on the cervical location should have been chosen.
ConclusionWe report a very rare case of chondrosarcoma metastasis to the thyroid gland. As in the few other cases reported in the literature, it appeared many years after the primary cancer. Thyroid metastases of chondrosarcoma or other cancers are generally associated with other metastatic lesions and, as in the other case reports, the patient rapidly died of multiple metastases. This emphasizes the fact that chondrosarcoma patients, even when successfully treated in the past, must always be treated cautiously when presenting a mass. Also, other metastatic sites, especially the lung, must be actively sought.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to express their sincere gratitude to Yves-Marie Robin of the Oscar Lambret Center in Lille for confirming the histopathological diagnosis.
Please cite this article as: Simon F, Classe M, Vironneau P, Wassef M, Herman P, Le Clerc N. Thyroid compressive mass, a metastasis of femur chondrosarcoma after 14 years: case report and literature review. Braz J Otorhinolaryngol. 2017;83:602–4.
Peer Review under the responsibility of Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial.
gology is pleased to honor the reviewers


