
The most common pathogen in bacterial pharyngotonsillitis is group A β-hemolytic streptococcus, although groups B, C, F,and G have also been associated with pharyngotonsillitis.
ObjectiveTo assess the levels of the cytokines TNF-α, IL-6,IL-4, and IL-10 in bacterial pharyngotonsillitis caused by group A and non-A (groups B, C, F and G) β-hemolytic streptococcus.
MethodsThe study was conducted at a pediatric emergency care unit. The sample comprised children (5–9 years old) with acute bacterial pharyngotonsillitis diagnosed between December of 2011 and May of 2012. The research involved collection of blood samples from the patients, enzyme-linked immunosorbent assay detection of TNF-α, IL-6,IL-4, and IL-10, and collection of two oropharyngeal swabs for bacterial isolation. Additionally, the medical history of the study participants was also collected.
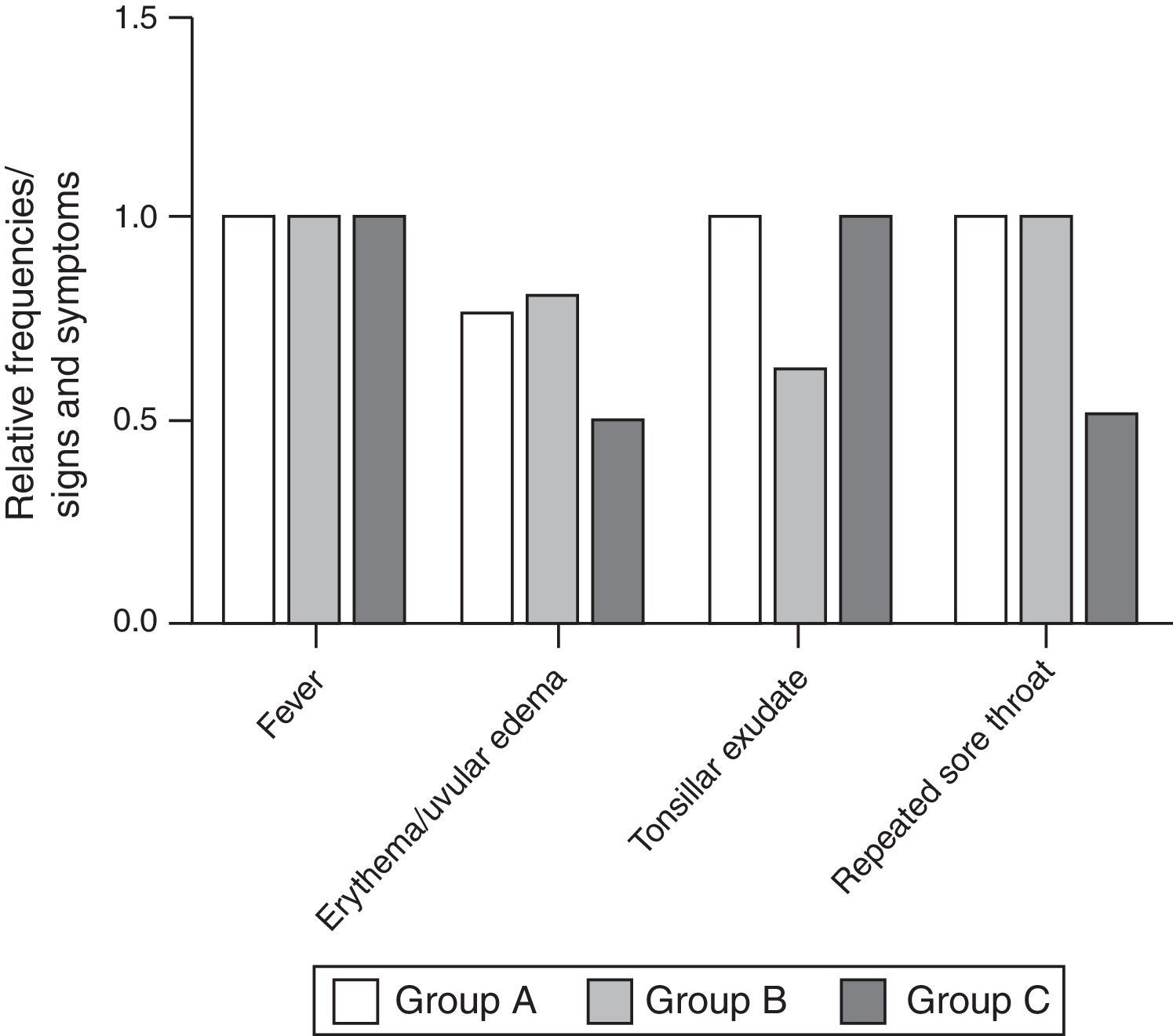
ResultsIn the studied group (mean age: 5.93 years), higher pharyngotonsillitis incidence was observed in the female gender (64.76%). Higher incidence of tonsillar exudates was observed with groups A and C. No statistically significant differences in cytokine levels were observed among groups. However, the group A and the control group showed a difference in the IL-6 level (p=0.0016).
ConclusionsThe Groups A and C showed higher cytokine levels than the Groups B and control, suggesting similar immunological patterns.
O patógeno mais comumente associado à faringotonsilite bacteriana é o estreptococo β-hemolíticodo grupo A, a despeito dos grupos B, C, F e G terem também sido associados coma faringotonsilite.
ObjetivoDeterminar os níveis das citosinas TNF-α, IL-6, IL-4, e IL-10 na faringotonsilite bacteriana causada pelos estreptococos β-hemolíticos do grupo A e não-A (grupos B, C, F e G).
MétodoO estudo foi conduzido em uma emergência pediátrica. A amostra estudada compreendeu crianças (entre 5 e 9 anos) com faringotonsilite aguda bacteriana diagnosticada entre dezembro de 2011 e maio de 2012. A pesquisa envolveu a coleta de amostras sanguíneas dos pacientes, a detecção, através do ELISA, de TNF-α, IL-6, IL-4 e IL-10, além da coleta de dois swabs orofaríngeos para isolamento bacteriano. Adicionalmente foi coletada a história médica dos participantes do estudo.
ResultadosNo grupo estudado (idade média: 5,93 anos), a maior incidência de faringotonsilites foi observada no gênero feminino (64,76%). Foram detectadas maiores incidências de exsudatos tonsilares nos grupos A e C. Não foram observadas diferenças estatisticamente significantes dos níveis de citosinas entre os grupos. Porém os grupos A e o controle mostraram diferença nos níveis de IL-6 (p=0.0016).
ConclusõesOs grupos A e C mostraram maiores níveis de citosinas que os grupos B e o controle, sugerindo mecanismos imunológicos similares.
Acute pharyngotonsillitis (PT) is one of the most common conditions observed by pediatricians, otorhinolaryngologists, and primary care physicians in their daily practice. It is estimated that >50% of cases of PT are of viral origin; among the bacterial cases, the most common pathogen is group A β-hemolytic streptococcus (GAS).1–3 However, β-hemolytic streptococci groups B, C, F, and G (especially C and G) can also cause self-limiting PT with non-suppurative sequelae, such as rheumatic fever.4,5
In the last 50 years, the overall incidence of bacterial PT caused by groups B, C, F, and G has increased. A 2011 study on the prevalence of β-hemolytic streptococci groups C and F in patients with acute pharyngitis demonstrated that these microorganisms cause PT in 6.2% of all cases of acute streptococcal infections.6–8
In turn, groups C and G streptococci (GCS and GGS) have been described as pyogenes-like, as these organisms share important virulence factors such as hemolysins, streptolysin O, extracellular enzymes, and M proteins, similar to GAS. They can also cause exudative isolated PT in addition to cellulitis, thus becoming clinically indistinguishable from GAS. Previous studies demonstrated that GCS causes a strong immunological response, as can be observed from the increase in antistreptolysin O (ASO) titer during streptococcal infection of the oropharynx.9–11 GBS also shows virulence factors similar to the GAS, including hemolysins, encapsulated polysaccharides, and C5a peptidase; hyaluronidase may also appear in some strains.12
Considering the abovementioned data on the shared virulence factors and clinically similar PT development, especially among groups A, C and G, this study aimed to assess the levels of TNF-α, IL-6, IL-4, and IL-10 cytokines in patients with PT, in order to distinguish pharyngotonsillitis caused by GAS from non-GAS.
MethodsThe study was carried out at an emergency unit of the city of Aracaju. The study population included children (5–9 years old) with acute bacterial PT diagnosed between December 2011 and May 2012.
Sample size calculation was performed considering the overall incidence of acute PT, which according to Simões et al. (2002) in a study carried out in Portugal, was 3440.3/105 for the age group of 5–9 years.6 The population of children in this age group in the city of Aracaju is 40,442 inhabitants, according to the 2010 Census (Brazilian Institute of Geography and Statistics – IBGE, 2012). Applying the incidence reported by the abovementioned study, using the formula for sample size calculation for a finite population – chi-squared – a sample of 50 children was attained.
The control group consisted of 25% of the total sample (12 patients) and was selected among the children accompanied by adults (relatives) who were admitted to the emergency room due to conditions unrelated to respiratory diseases. The accompanying children were declared healthy by their parents.
The inclusion criteria were the following:
- (1)
Diagnostic hypothesis of bacterial PT demonstrated by at least two symptoms: sudden odynophagia, fever, headache, nausea, vomiting and abdominal pain, pharyngotonsillar inflammation, palatal petechiae, anterior cervical adenitis, and scarlatiniform rash.
- (2)
No history of cardiovascular disease.
- (3)
Resident of the municipality of Aracaju.
Patients with suspected viral PT, with the following symptoms: conjunctivitis, rhinitis, cough, diarrhea, hoarseness, mild ulcerative stomatitis, and viral rash were excluded.13
The study was divided into two phases: the first consisted of blood sample collection from patients with a diagnostic hypothesis of bacterial acute PT, to perform the enzyme-linked immunosorbent assay (ELISA) test for TNF-α, IL-6, IL-4, and IL-10 cytokines, plus collection of two oropharynx swabs for bacterial isolation, seeded on a petri dish containing blood agar. The second phase consisted of individual inquiry, which contained data on socioeconomic status and the child's health history.
Microbiological phaseThe methodology for the microbiological phase of the study was described based on Modules III and V of Clinical Microbiology Manual for Infection Control in Health Services by the Brazilian National Health Surveillance Agency (Agência Nacional de Vigilância Sanitária [ANVISA]), concerning the microbiological laboratory procedures and identification of medically important bacteria, respectively.14
The oropharyngeal swabs were collected following the technique described by Levy et al. (2004) to obtain a culture specimen for Streptococcus sp. isolation. The technique followed the sequence described: the patient was asked to open his/her mouth; using a tongue depressor and sterile swabs, smears were obtained from the tonsils and posterior pharynx, seeking to collect the material from the areas closest to the sites of suppuration and avoiding other oral cavity sites.14
For the presumptive identification of colonies of beta-hemolytic streptococci, the specimens were seeded on a petri dish containing blood agar using aseptic techniques and incubated for 24h in a bacteriological incubator, using the candle-jar technique at 35°±2°C. After incubation, the colonies were tested with catalase to eliminate Microccocacea (staphylococci), which generally give a positive result for catalase activity, whereas streptococci, in general, yield a negative catalase test. As evidential test, Gram stain was performed in catalase-negative colonies, with subsequent visualization of the morphological and color appearance of the specimens under optical microscopy with oil immersion.
After the microscopic confirmation of streptococci, a co-agglutination test using Phadebact® Strep AD, F, and G Test – Bactus AB Test® was performed. The colonies of β-hemolytic group A streptococci (Streptococcus pyogenes) were identified using bacitracin at a concentration of 0.04IU, with the formation of an inhibition zone as a result of sensitivity.
Serological phaseBlood samples (4mL) collected from each patient were maintained in serum separator tubes and centrifuged at 5000rpm for 15min, with the serum separated into three aliquots of 500μL and stored at −80°C. The ELISA technique was performed for all cytokines according to the manufacturer's instructions (ELISA Ready-SET-Go!® – EBIOSCIENCE). Serum cytokine concentrations were measured in pg/mL using standard curves previously described by the manufacturer: IL-4 (2–200pg/mL); IL-6 (2–200pg/mL); IL-10 (2–300pg/mL); and TNF-α (2–200pg/mL).
The C-reactive protein (CRP) measurement technique was performed according to the manufacturer (Turbilátex kit – BIOTÉCNICA). Essentially, the method consists of the agglutination of latex particles coated with human anti-CRP antibody by the C-reactive protein (CRP) present in the sample. The agglutination causes an increase in absorbance proportional to the concentration of CRP in the sample, and by comparison with a known concentration of CRP calibrator, the content of the CRP in the assayed sample at 540nm can be determined.
Statistical analysisThe data were stored in a database in a Microsoft Excel spreadsheet. For comparison of the studied cytokines, as well as signs and symptoms between groups, this study used ANOVA and the Kruskal–Wallis test with Bonferroni's and Dunn's post-tests, respectively, with 95% confidence interval. Data were analyzed using GraphPad-Prisma5 software (GraphPad Software – San Diego, CA, United States).
EthicsThis research protocol was approved by the Research Ethics Committee of Universidade Federal de Sergipe (CEP), under No. CAAE 0098.0.107.000-11.
ResultsThe study population consisted of 74 patients (62 symptomatic and 12 controls) aged 5–9 years (mean age 5.93±1.69 years). Regarding gender, 69.76% of the sample consisted of females (p=0.03).
Regarding microbiological findings, it was observed that α-hemolytic streptococci were present in 46.55% of the studied population. B-hemolytic colonies were isolated from 36.21% of the samples. Of these isolates, 47.61% were catalase-positive, presumably Staphylococcus aureus, while 52.39% were catalase-negative, presumably Streptococcus sp. Catalase-negative isolates were further tested using the latex co-agglutination test and these test results were used to subdivide beta-hemolytic streptococci into Lancefield groups A, B, and C; other groups were not detected among the samples. As for the different groups, GAS showed an incidence of 36% among the isolated streptococcal samples, whereas the incidence of GCS and GBS was 18% and 46% among the isolates, respectively.
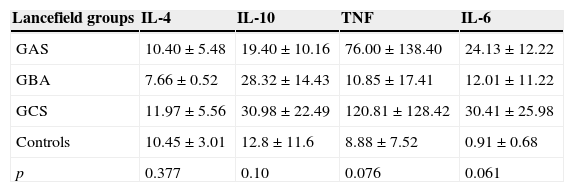
As for serum cytokines among the different groups of beta-hemolytic streptococci, it was observed that IL-6 levels (pg/mL) were significantly higher in group A than in controls (p=0.0016). Although it did not show significantly higher levels when compared to other groups, mean GCS was significantly higher (30.41±25.98pg/mL), even greater than that shown by GAS (24.13±12.22pg/mL). Mean levels of GBS were higher than controls, indicating active infection; however, these levels were 2- to 2.5-fold lower than those shown by GAS and CGS, respectively (Table 1).
Comparison of levels of cytokines (pg/mL) in different groups of β-hemolytic streptococci by analysis of variance.
| Lancefield groups | IL-4 | IL-10 | TNF | IL-6 |
|---|---|---|---|---|
| GAS | 10.40±5.48 | 19.40±10.16 | 76.00±138.40 | 24.13±12.22 |
| GBA | 7.66±0.52 | 28.32±14.43 | 10.85±17.41 | 12.01±11.22 |
| GCS | 11.97±5.56 | 30.98±22.49 | 120.81±128.42 | 30.41±25.98 |
| Controls | 10.45±3.01 | 12.8±11.6 | 8.88±7.52 | 0.91±0.68 |
| p | 0.377 | 0.10 | 0.076 | 0.061 |
Reference levels: IL-4 (0–38.7pg/mL); IL-6 (0–5.9pg/mL); IL-10 (1.5–9.1pg/mL); and TNFα (0–20pg/mL).
A similar result was observed for the quantification of TNF-α, which did not significantly differ between groups, although GAS and GCS showed higher levels than GBS, which were similar to the control group. The levels of anti-inflammatory cytokines IL-4 and IL-10 were also measured, but showed no statistically significant differences between the groups, including the control group (Table 1).
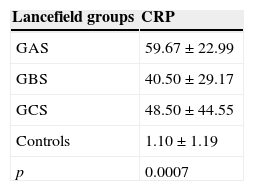
Due to a significant increase in IL-6 levels caused by GAS infections, CRP levels were also measured, which showed a significant increase in levels of β-hemolytic streptococci in relation to the control group (p=0.0007); however, statistically significant differences were not observed between the groups, although the mean levels in the GAS group were higher than in the others, suggesting that GAS leads to a more intense inflammatory response (Table 2).
DiscussionThe development and regulation of an autoimmune response depend on cytokine production and release, that can determine the differentiation of antigen-specific T cells in an appropriate effector T-cell lineage. The immune response to infection is regulated by the balance between the mechanisms inducing the production of Th1 and Th2 cytokines. The cytokines derived from Th1 (IL-2 and IFN-γ) induce an immune response through a cell-dependent pathway, while cytokines derived from the Th2 type (IL-4) suppress cell-mediated response pathway and induce humoral response, which involves the release of IL-4, IL-5, IL-6, and IL-10.15,16
In this study, the measurement of levels of IL-4, IL-6, IL-10, and TNF-α cytokines in children with acute pharyngotonsillitis caused by beta-hemolytic streptococci showed high levels of pro-inflammatory cytokines IL-6 and TNF-α. However, the levels of anti-inflammatory cytokines, especially IL-4, were similar to those found in the control group, suggesting a change in immune response mediated by Th1.
The levels of pro-inflammatory cytokines in the GAS and GCS groups showed higher mean values than those in the GBS and control groups; similarly, the mean anti-inflammatory cytokine levels were higher in GAS and GCS groups, suggesting similar immunological mechanisms. Aiming to assess the degree of homeostasis between the production of pro-inflammatory cytokines and anti-inflammatory factors, the ratio of TNF-α in relation to IL-4 and IL-10 anti-inflammatory cytokines was calculated. The proportion was higher for the infection caused by GCS, suggesting a tendency toward more acute immune and inflammatory responses, with a change to Th1 pattern.16
Cytokines levels reflect the manifestation of signs and symptoms. More aggressive manifestations were observed in patients with PT caused by GAS and GCS groups when compared to those caused by GBS, especially in relation to tonsillar exudates (Fig. 1). PTs caused by GBS usually show lower levels of pro-inflammatory cytokines when compared to levels found in other groups; these data suggest a weaker immune response to virulence factors of this group, reflecting milder clinical manifestations15 (Fig. 1).
 and C (GCS).")
IL-6 levels in the serum of children with PT caused by beta-hemolytic streptococci increased between the different groups when compared to the control group. IL-6 stimulates hepatocytes to produce high levels of acute-phase proteins such as C-reactive protein (CRP) during active infection or acute inflammatory process, giving it the status of inflammatory marker.17–19 In this study, mean CRP levels in GAS were higher than in the other groups, suggesting a more intense inflammatory response (Table 2).
Although GAS and GCS share virulence factors such as M protein, which is considered the main factor responsible for the virulence and pathogenesis of acute rheumatic fever, GCS is not related to this non-suppurative complication and can only be associated with acute glomerulonephritis.4,9 However, in opposition to this information, Haidan et al. (2000) showed that in cases of PT caused by GBS and GGS groups in an aboriginal population there was a higher incidence of rheumatic fever, as well as a low incidence of GAS infection, suggesting that, in vitro, GBS and GGS, under specific circumstances, have the potential to initiate an autoimmune response, which could emulate a picture of acute rheumatic fever.20–22 This finding indicates the clinical importance of this bacterium and also that it is appropriate to investigate and treat PT cases caused by GCS, as well as by GAS.
ConclusionIt can be concluded that PT caused by GAS, GBS, and GCS showed representative incidences and similar signs and symptoms. However, PT caused by GAS and GCS are more acute, as demonstrated by the immune response and the high levels of pro-inflammatory cytokines, suggesting that immunological mechanisms are similar in the two groups.23,24 This similar immune response in these circumstances could be attributed to shared virulence factors, such as M protein and streptolysin O. GBS identified in this study also caused PT in children, although it induced less aggressive immune and clinical responses than GAS and GCS.
FundingThis study was supported by CNPq (Conselho Nacional de Desenvolvimento Cientifico e Tecnologico,Brasília, DF, Brazil) and FAPITEC (Fundação de Apoio à Pesquisa e à Inovação Tecnológica de Sergipe, Aracaju, SE, Brazil).
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Leão SC, Leal IO, Rocha HMN, Rodrigues TMA. Evaluation of cytokines produced by β-hemolytic streptococcus in acute pharyngotonsillitis. Braz J Otorhinolaryngol. 2015;81:402–7.
Institution: Molecular Anatomy Group, Department of Morphology, Universidade Federal de Sergipe (UFS), São Cristóvão, SE, Brazil.
gology tem o prazer em homenagear os revisores


