
In order to meet the demands of the patient population with hearing impairment, the Hearing Health Care Network was created, consisting of primary care actions of medium and high complexity. Spatial analysis through geoprocessing is a way to understand the organization of such services.
ObjectiveTo analyze the organization of the Hearing Health Care Network of the State of Minas Gerais.
MethodsCross-sectional analytical study using geoprocessing techniques. The absolute frequency and the frequency per 1000 inhabitants of the following variables were analyzed: assessment and diagnosis, selection and adaptation of hearing aids, follow-up, and speech therapy. The spatial analysis unit was the health micro-region.
ResultsThe assessment and diagnosis, selection, and adaptation of hearing aids and follow-up had a higher absolute number in the micro-regions with hearing health services. The follow-up procedure showed the lowest occurrence. Speech therapy showed higher occurrence in the state, both in absolute numbers, as well as per population.
ConclusionThe use of geoprocessing techniques allowed the identification of the care flow as a function of the procedure performance frequency, population concentration, and territory distribution. All procedures offered by the Hearing Health Care Network are performed for users of all micro-regions of the state.
Para atender às demandas da população com deficiência auditiva, o SUS criou as Redes Estaduais de Atenção à Saúde Auditiva, compostas por ações na atenção básica, média e alta complexidade. Uma forma de se compreender a organização desses serviços nos territórios de saúde é utilizando-se análise espacial, realizada por meio do geoprocessamento.
ObjetivoAnalisar a organização da Rede Estadual de Atenção à Saúde Auditiva em Minas Gerais.
MétodoEstudo analítico transversal, utilizando-se técnicas de geoprocessamento. Foram analisadas a frequência absoluta e frequência por mil habitantes das variáveis: avaliação e diagnóstico, seleção e adaptação de AASI, acompanhamento e terapia fonoaudiológica. A unidade de análise espacial foi a microrregião de saúde.
ResultadosOs procedimentos avaliação e diagnóstico, seleção e adaptação de AASI e acompanhamento tiveram maior número absoluto nas microrregiões onde há Serviços de Saúde Auditiva credenciados. O procedimento de acompanhamento apresentou a menor ocorrência no Estado. O procedimento terapia fonoaudiológica apresentou maior ocorrência, tanto em valor absoluto quanto por população.
ConclusãoA utilização do geoprocessamento permitiu identificar o fluxo do atendimento em função da frequência de realização dos procedimentos, concentração populacional e distribuição territorial. Todos os procedimentos analisados são realizados em usuários em todas as microrregiões do Estado.
Hearing loss characterizes a sensory deficit that limits the subject's performance at any age and has adverse effects on quality of life, cognitive function, and on the emotional, behavioral, and social well-being.1,2
According to data from the World Health Organization (WHO), hearing loss is the third most common disability in Brazil. Half of all cases of hearing loss are avoidable through prevention, early diagnosis, and management procedures.3 To meet the demands of this population, one of the strategies of the health care system was the creation of a State Hearing Health Network in the Brazilian Unified Health System (Sistema Único de Saúde – SUS), established by Ministerial Decree No. 587 of October 7, 2004, which determines the organization and implementation of actions in primary care by medium and high-complexity care services in these networks. These actions seek to offer an integrated approach to care, hearing health promotion, prevention, and early identification of hearing problems in the community, as well as informational and educational services, family counseling, and referrals to the Hearing Health Service.4
Considering the recent process of creation of this policy, the evaluation of health initiatives gains importance in the sector,5 as it provides relevant information to the process of decision-making based on evidence.6 One way to understand how these services are organized in the territories of healthcare is to use spatial analysis of the elements that comprise the care network, conducted by means of geoprocessing, a set of technologies that analyzes and evaluates information regarding a geographical space with a certain objective.7
For such purposes, it is necessary to establish the geographical location of events, associating graphical information (maps) to the health database and using tools to manipulate spatially presented information.8 Among the many information systems, a geographic information system (GIS) facilitates the collection, storage, manipulation, analysis, visualization, and production of geographically referenced data,9 allowing the qualification and organization of health services according to the particularities of each geographic area,10 which contributes to a better understanding of current health problems.
Geoprocessing techniques have been applied to public and collective health, as they allow analyzing the associations between environment and health-related events, assisting the planning, monitoring, and evaluation of health actions and contributing to the structuring and analysis of environmental risks.8,11 Moreover, the use of such techniques aims to spatially identify areas with specific characteristics in order to subsidize programs or policies aimed at health care improvement, increasing the efficiency of the use of public resources and defining priority areas.12
The present study aimed to analyze the organization of the State Hearing Health Network in the health micro-regions of the state of Minas Gerais and assess the spatial pattern between procedures of evaluation and diagnosis, selection and adaptation of the individual sound amplification device (ISAD), follow-up, and speech/audiological therapy performed at health care services.
MethodsThe present study is part of the project “Evaluation of the Hearing Health Network Implementation: A case study of the micro-regions of Sete Lagoas and Curvelo, Minas Gerais”, funded by the Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG) and approved by the Ethics Committee of the institution under No. ETIC 186-10.
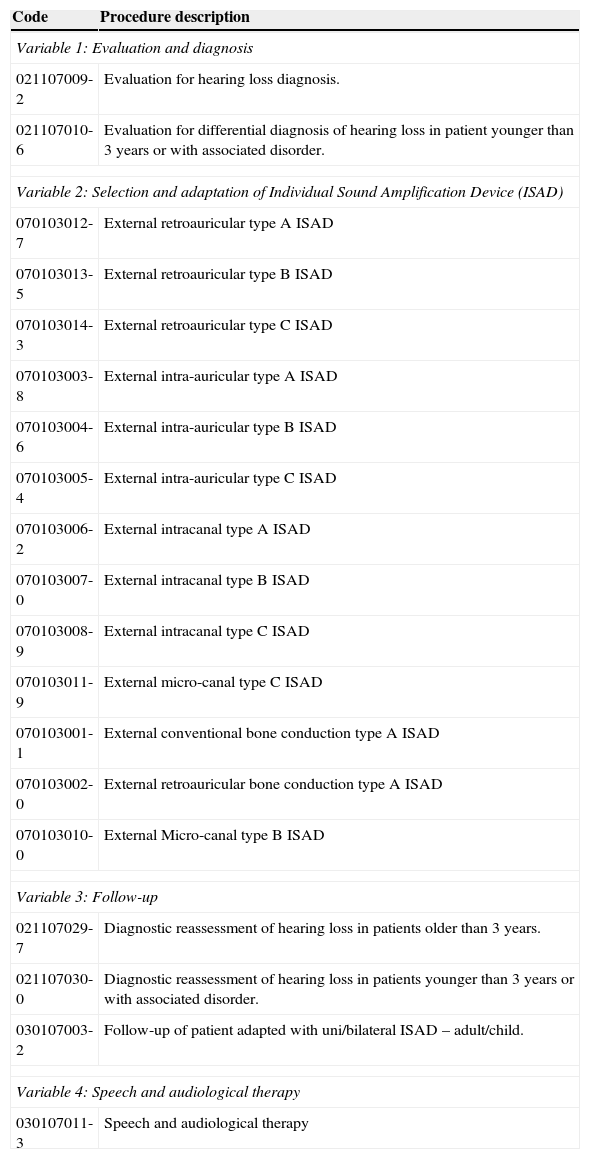
This is a cross-sectional analytical study using geoprocessing techniques. Data from the Outpatient Information System (SIA/SUS) were used for the construction of variables per health micro- and macro-region, considering the Master Plan for Regionalization of the state of Minas Gerais and the city of residence of the network users. The following variables were used: evaluation and diagnosis, selection and adaptation of the ISAD, follow-up, and speech/audiological therapy for the year 2010 (Table 1), to allow the assessment of the patients itinerary at the main points of the care network.
Description of procedures considered for calculation of the study variables.
| Code | Procedure description |
|---|---|
| Variable 1: Evaluation and diagnosis | |
| 021107009-2 | Evaluation for hearing loss diagnosis. |
| 021107010-6 | Evaluation for differential diagnosis of hearing loss in patient younger than 3 years or with associated disorder. |
| Variable 2: Selection and adaptation of Individual Sound Amplification Device (ISAD) | |
| 070103012-7 | External retroauricular type A ISAD |
| 070103013-5 | External retroauricular type B ISAD |
| 070103014-3 | External retroauricular type C ISAD |
| 070103003-8 | External intra-auricular type A ISAD |
| 070103004-6 | External intra-auricular type B ISAD |
| 070103005-4 | External intra-auricular type C ISAD |
| 070103006-2 | External intracanal type A ISAD |
| 070103007-0 | External intracanal type B ISAD |
| 070103008-9 | External intracanal type C ISAD |
| 070103011-9 | External micro-canal type C ISAD |
| 070103001-1 | External conventional bone conduction type A ISAD |
| 070103002-0 | External retroauricular bone conduction type A ISAD |
| 070103010-0 | External Micro-canal type B ISAD |
| Variable 3: Follow-up | |
| 021107029-7 | Diagnostic reassessment of hearing loss in patients older than 3 years. |
| 021107030-0 | Diagnostic reassessment of hearing loss in patients younger than 3 years or with associated disorder. |
| 030107003-2 | Follow-up of patient adapted with uni/bilateral ISAD – adult/child. |
| Variable 4: Speech and audiological therapy | |
| 030107011-3 | Speech and audiological therapy |
These variables were subsequently converted into indicators by incorporating the relative population variation to the original data magnitude, using data from the 2010 census by the Instituto Brasileiro de Geografia e Estatística (IBGE). The variables represented in choropleth maps were comprehended from six class intervals defined by a natural breaks distribution, which establishes the interval limits using actual breaks in the histogram through visualization by the researchers. After the representation of variables as indexes (1000 inhabitants/year), a specific cartographic representation of the absolute frequency was established. This methodological procedure used four class intervals, also defined by the method of natural breaks distribution.
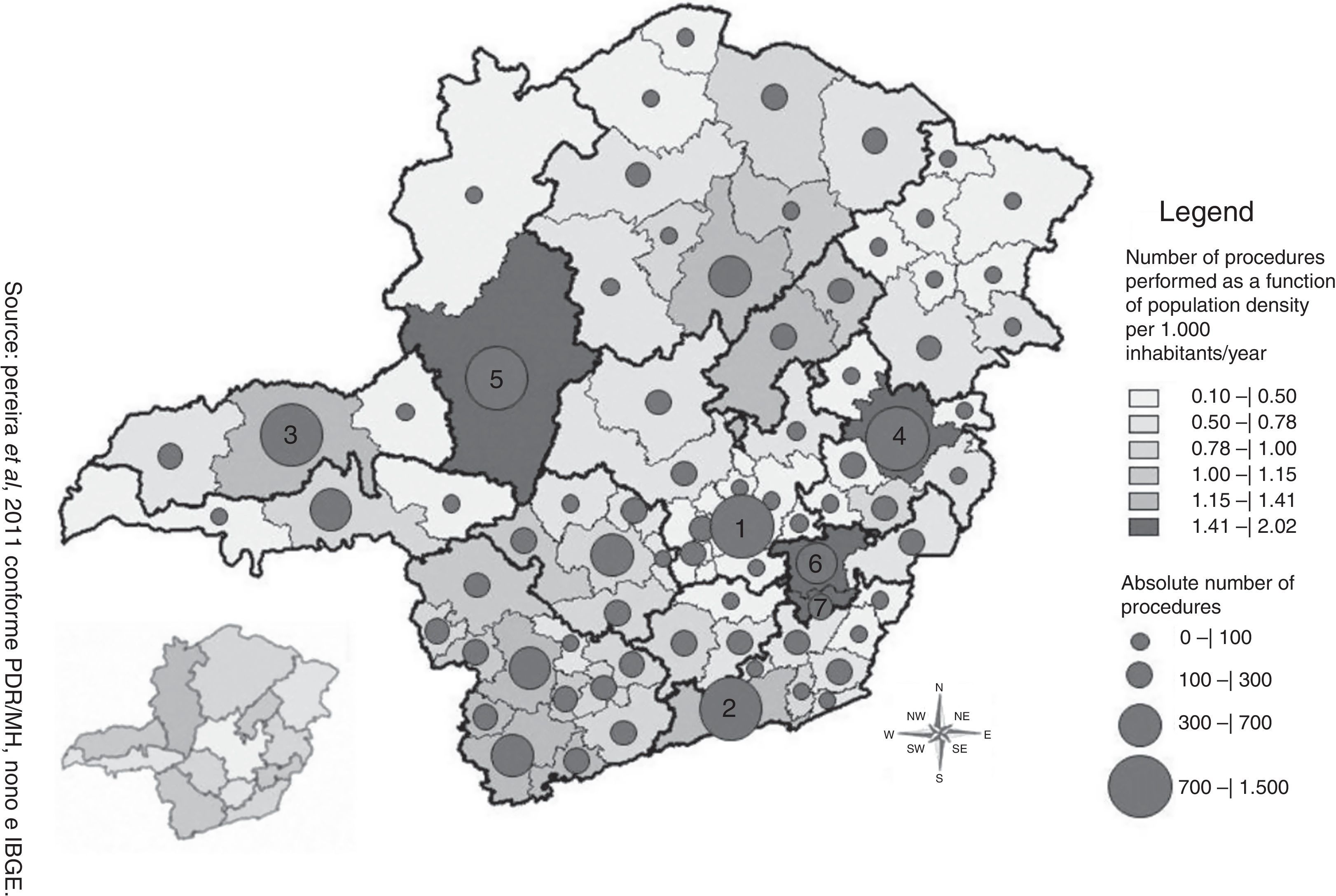
ResultsIn 2010, the state of Minas Gerais had 15 accredited Hearing Health Services, distributed over 14 micro-regions, of which eight are highly complexity (located in the municipalities of Belo Horizonte, Uberlândia, Alfenas, Pouso Alegre, Montes Claros, Governador Valadares, Ponte Nova, and Juiz de Fora) and seven are medium complexity (located in the municipalities of Formiga, Santa Luzia, Uberaba, Patos de Minas, Diamantina, and Teofilo Otoni). All procedures analyzed in all state health micro-regions were performed, although the frequency of occurrence was not homogeneous throughout the territory, mainly when comparing the four moments of care provided to patients in the network (from diagnosis to speech/audiological therapy) (Figs. 1–4).




The variable evaluation and diagnosis occurred at higher absolute frequency in the micro-regions of Belo Horizonte/Nova Lima/Caeté, Juiz de Fora/Lima Duarte/Bom Jardim Minas, Uberlândia/Araguari, Governador Valadares, and Patos de Minas, and the latter two also had a greater number of individuals who underwent this procedure, together with the micro-regions of Ponte Nova and Viçosa. Although it showed a higher value of absolute frequency of evaluations and diagnoses, the micro-region of Belo Horizonte/Nova Lima/Caeté was indicated on the map as one of the micro-regions with lower value per population that performed such procedures (Fig. 1).
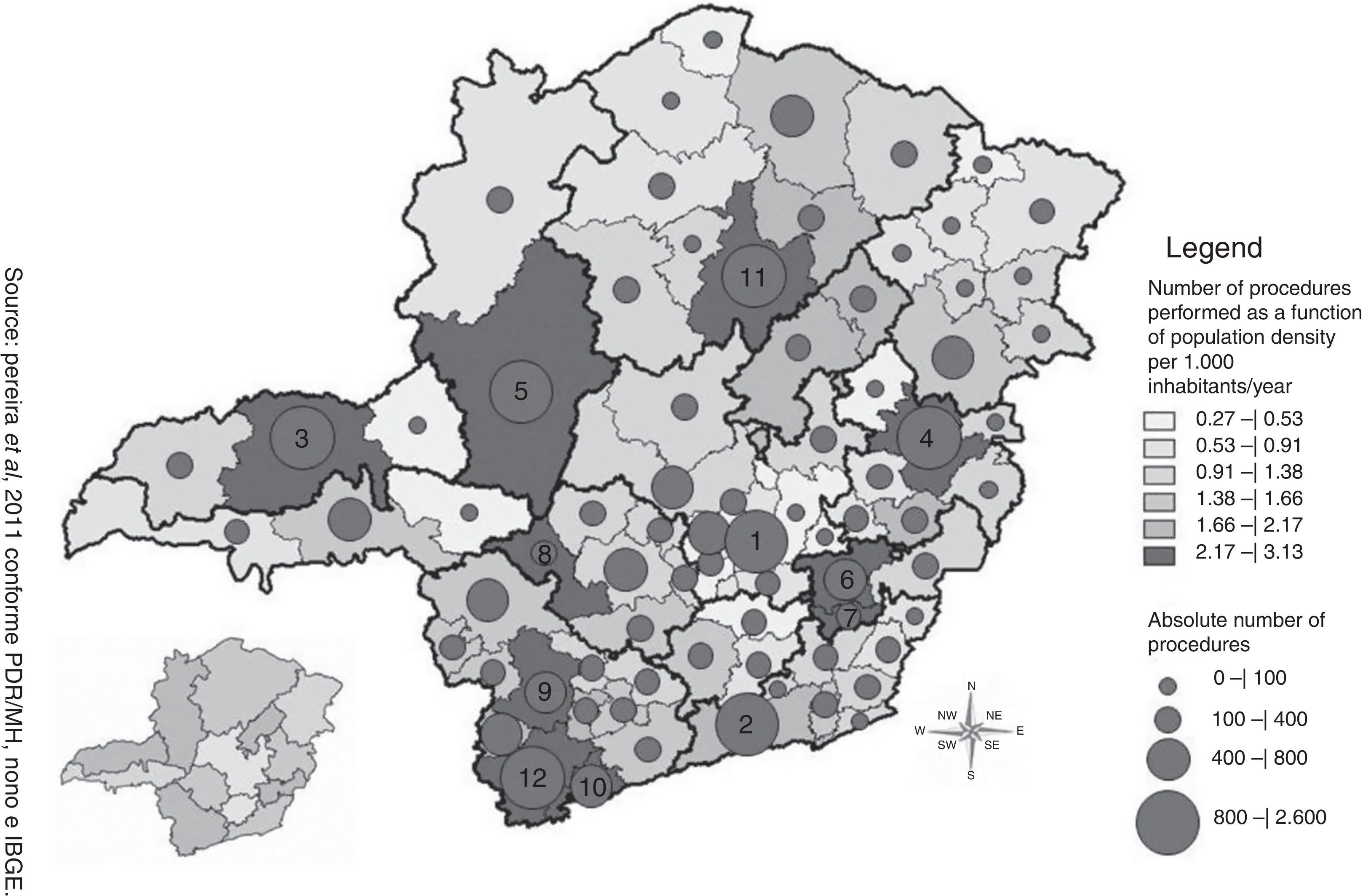
The spatial distribution of the procedure “selection and adaptation of the ISAD” showed a higher number of procedures as a function of population density per 1000 inhabitants in the micro-regions of Ponte Nova, Viçosa, Formiga, Alfenas/Machado, Itajubá, Governador Valadares, Patos de Minas, Montes Claros/Bocaiúva, Pouso Alegre, and Uberlândia/Araguari. Of these, only the last five also had higher absolute frequency value of this procedure. In addition to the abovementioned, the micro-regions of Belo Horizonte/Nova Lima/Caeté and Juiz de Fora/Lima Duarte/Bom Jardim Minas showed a high absolute frequency value for selection and adaptation of ISAD performed in 2010. A higher number per 1000 inhabitants and absolute frequency of this procedure was observed between the micro-regions when compared to the variable evaluation and diagnosis (Fig. 2).
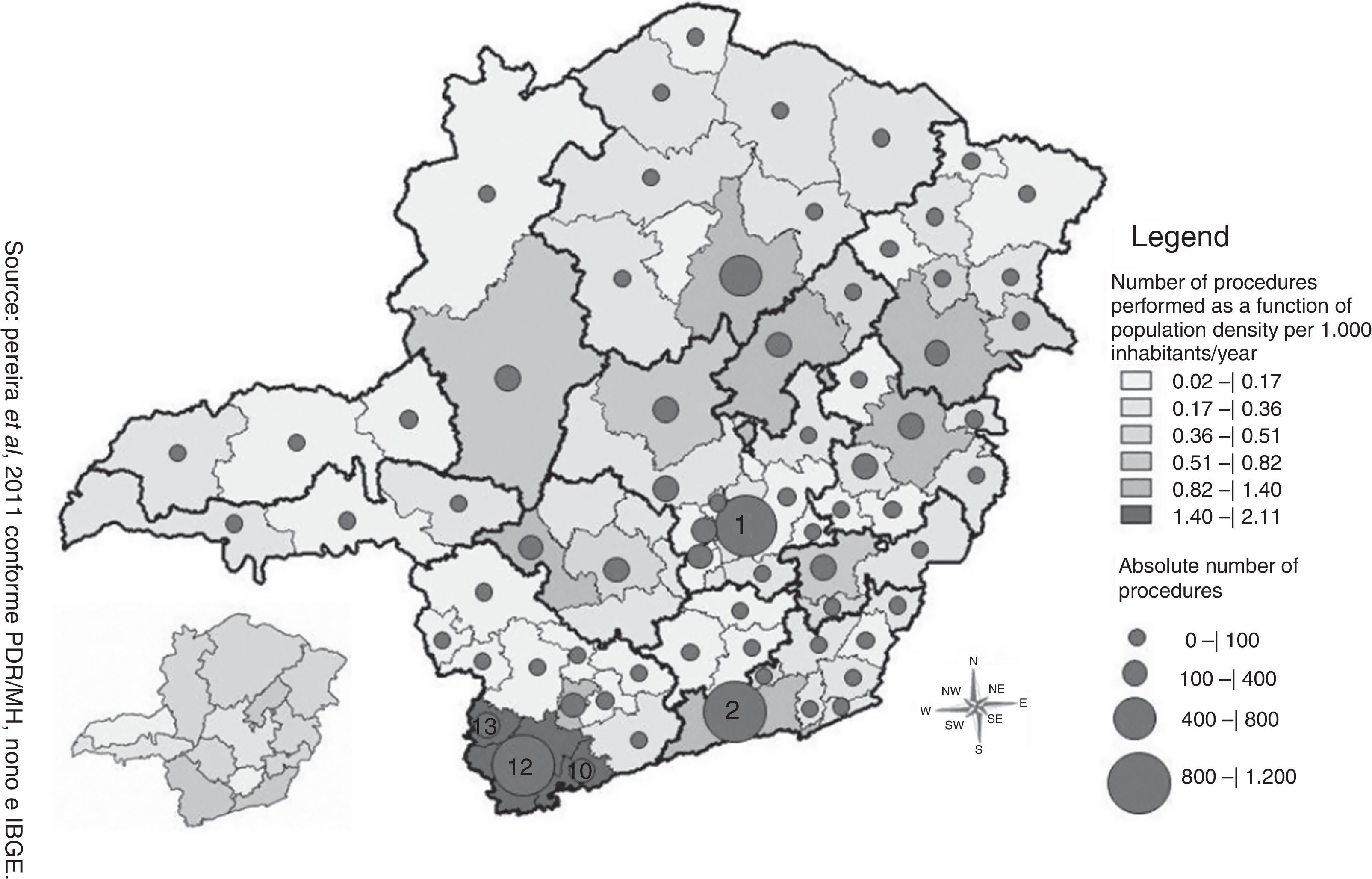
The follow-up procedure occurred at the highest absolute frequency in the regions of Belo Horizonte/Nova Lima/Caeté, Juiz de Fora/Lima Duarte/Bom Jardim Minas, and Pouso Alegre, whereas the micro-regions of Itajubá, Pocos de Caldas, and Pouso Alegre showed higher value per population submitted to such procedure. The map demonstrated large areas with low production of this procedure per 1000 inhabitants, as well as low values of absolute frequency of this procedure, with this variable showing the lowest occurrence in the state (Fig. 3).
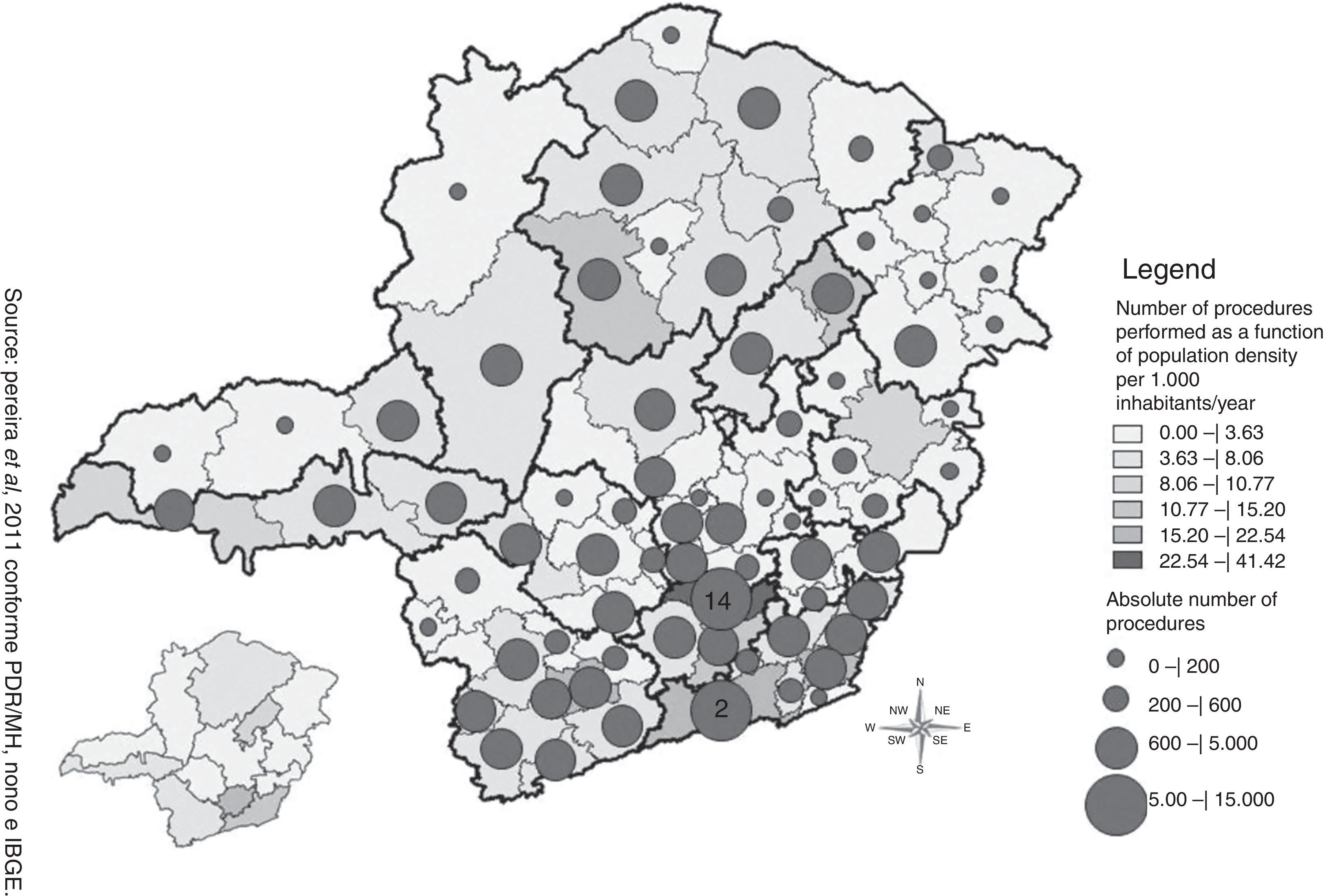
The speech/audiological therapy procedure occurred at greater absolute numbers in the regions of Juiz de Fora/Lima Duarte/Bom Jardim Minas and Conselheiro Lafaiete/Congonhas, with the latter being the only micro-region highlighted per population. The map showed that this procedure occurred at greatest frequency per 1000 inhabitants, and its maximum value was 41.42 speech/audiological therapy sessions/1000 inhabitants (Fig. 4).
A directly proportional association was not observed between the absolute number of procedures of the analyzed variables and the number of procedures per 1000 inhabitants, i.e., the health regions with higher production related to the variables did not necessarily have a higher number of procedures in relation to population. Moreover, no micro-region was highlighted regarding all analyzed variables.
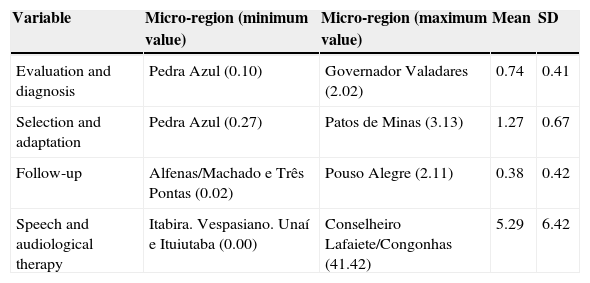
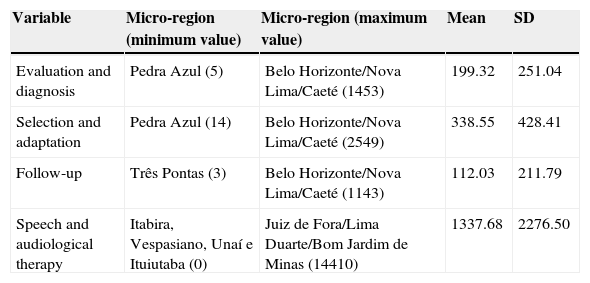
Tables 2 and 3 show the minimum, maximum, mean, and standard deviation values for each analyzed variable and their respective micro-region of occurrence regarding the number of procedures as a function of population density per 1000 inhabitants/year and the absolute number of procedures, respectively.
Minimum, maximum, mean, and standard deviation values as a function of the number of procedures performed considering the demographic density of 1000 inhabitants/year in the state of Minas Gerais.
| Variable | Micro-region (minimum value) | Micro-region (maximum value) | Mean | SD |
|---|---|---|---|---|
| Evaluation and diagnosis | Pedra Azul (0.10) | Governador Valadares (2.02) | 0.74 | 0.41 |
| Selection and adaptation | Pedra Azul (0.27) | Patos de Minas (3.13) | 1.27 | 0.67 |
| Follow-up | Alfenas/Machado e Três Pontas (0.02) | Pouso Alegre (2.11) | 0.38 | 0.42 |
| Speech and audiological therapy | Itabira. Vespasiano. Unaí e Ituiutaba (0.00) | Conselheiro Lafaiete/Congonhas (41.42) | 5.29 | 6.42 |
SD, standard deviation.
Minimum, maximum, mean, and standard deviation values as a function of the absolute number of procedures performed in the state of Minas Gerais.
| Variable | Micro-region (minimum value) | Micro-region (maximum value) | Mean | SD |
|---|---|---|---|---|
| Evaluation and diagnosis | Pedra Azul (5) | Belo Horizonte/Nova Lima/Caeté (1453) | 199.32 | 251.04 |
| Selection and adaptation | Pedra Azul (14) | Belo Horizonte/Nova Lima/Caeté (2549) | 338.55 | 428.41 |
| Follow-up | Três Pontas (3) | Belo Horizonte/Nova Lima/Caeté (1143) | 112.03 | 211.79 |
| Speech and audiological therapy | Itabira, Vespasiano, Unaí e Ituiutaba (0) | Juiz de Fora/Lima Duarte/Bom Jardim de Minas (14410) | 1337.68 | 2276.50 |
SD, standard deviation.
Albeit heterogeneously, all procedures related to the four moments of the hearing health care service were performed in users residing in all health micro-regions of the state. The principle of SUS regionalization guarantees that health services are organized into levels of increasing technological complexity, arranged in a delimited geographic area and aimed at a population to be treated.13 Thus, users should find secondary care services within the micro-region corresponding to the municipality of residence.14
Although all the health micro-regions demonstrated production, none showed significant production values per population at the four moments of care to individuals with hearing loss, as shown in Figs. 1–4. This may indicate that the Hearing Health Network is not fully implemented in any of the state micro-regions as recommended by the Ministerial Decree No. 587 of October 7, 2004. The form used by health managers for the purpose of accreditation of Middle and High-Complexity Audiology services4 evaluates structural issues that can be enough for qualification of centers, but can lead to erroneous conclusions when used as the sole instrument for accreditation of existing services, as this form does not evaluate the service performance in terms of providing the service and the demand for the service in the micro-region. Thus, there it is necessary to establish objective indicators to assess the level of implementation of the Hearing Health Network in the state micro-regions.
Although in 2010 the micro-region of Belo Horizonte/Nova Lima/Caeté was the only center that had two hearing healthcare services that were accredited and associated to educational institutions. This micro-region showed low values per population submitted to the procedure of assessment and diagnosis, in comparison to the other micro-regions.
The increase in the use of health services may be related to increased supply,15,16 which makes possible the existence of pent-up demands and needs suppressed by insufficient supply of public health actions and services. These data suggest the existence of a pent-up demand and an inadequate supply of services, considering the population of 3,186,312 inhabitants which was encompassed by this micro-region in 2010.
The micro-regions highlighted as those with the higher absolute number of evaluation and diagnosis, selection and adaptation of ISAD, and follow-up procedures are micro-regions that have middle- or high-complexity accredited Hearing Health Services, which may be due to easier access of users considering the shortest distances from the residence to the service. It is the responsibility of the municipality to ensure access of users undergoing outpatient treatment to other locations, when the municipality of origin does not offer the degree of complexity required by the user.13
However, the Health Care State Transportation System (SETS) offered by the Health Secretariat of Minas Gerais covered only 21 (27.63%) of the 76 micro-regions of the State in 2009. In 2010, it was predicted that 41 (53.94%) of the micro-regions would be covered by the SETS,17 which can make it difficult or even impossible for users to access Hearing Health Care services. Only the speech/audiological therapy procedure was also highlighted in the micro-region of Conselheiro Lafaiete/Congonhas, which does not have accreditation for this service. However, this fact is justified by the availability of speech/audiological therapy in a decentralized manner, which can be performed by the Municipal Hearing Health Referrals.18
The higher frequency of selections and adaptation of ISAD procedure in relation to the evaluation and diagnosis procedure can be justified considering that the most users with hearing loss undergo binaural ISAD adaptation, and so, in these cases, the procedure is considered twice for the same individual, whereas the assessment and diagnosis procedure is considered only once, regardless whether hearing loss is unilateral or bilateral.
However, the confirmation of this hypothesis is not possible, as the data provided in the Outpatient Information System show no separation regarding the selection and adaptation of monaural or binaural ISAD per user. Additionally, there is also the possibility that the user will undergo the evaluation and diagnosis procedure through a private health care service/insurance or private consultations, with interposition of users who use public and private services, as is the case of those patients who seek the health care center only to undergo vaccinations, according to their private physician's indication, but when they need medical consultations or examinations for diagnosis and therapeutic support, they use their health insurance.19
This study showed that follow-up is the procedure with the lowest occurrence in the state. Patient follow-up is essential for the effective use of ISAD and consequent success in its adaptation,20 which becomes feasible by means of periodic returns to the Hearing Health Program, aiming to monitor hearing loss and verify effectiveness of the ISAD use.4 It has been observed that outpatient visits related to patient follow-up have decreased over the years,21 with lower spontaneous rates of return for follow-up than the abandonment rates of the Health Hearing Program.22
Low patient adherence to the auditory rehabilitation process can be the result by several factors, such as lack of awareness about the fact that adaptation to the ISAD is only one step in the process, or the difficulty of access to the service, in cases of patients who need to undergo treatment at a service outside the city of residence.23 Additionally, the follow-up procedure should occur at least once a year; therefore, it is expected that it would occur at higher absolute frequency and in a larger number of the population.4 Although it is not sufficient, the active search for users of the Hearing Health Service for return consultations and follow-up procedures has been shown to be effective22 and can be an alternative to increase service adherence.
In contrast to the low number of follow-up procedures in the state, it was observed that speech/audiological therapy occurs frequently in all the regions, which is also observed at the national level, where 61.77% of the performed procedures refer to speech/audiological therapy, with a decrease in outpatient services related to follow-up observed over the years.21
The high value of occurrence per absolute frequency and per population of this procedure is justified by the fact that speech/audiological therapy can be indicated more than once, taking into account the individual characteristics and needs of the user, and also due to the possibility of performing this procedure according to the Hearing Health Municipal References,18 which reduces potential difficulties of access to the service. Such justifications also explain the higher value of this procedure in relation to other evaluated procedures.
Several factors, such as access, pent-up demand, and difficulty of treatment adherence, among other factors, seem to influence the way existing services are used by the population. These facts points to the need to better understand the association among these factors and the use of hearing health services, as well as to define process indicators that allow monitoring and evaluation of the network implementation process in the state.
It is necessary to conduct further evaluation studies of the Hearing Health Network, both at the state and the national level, in order to define areas and services that require greater resources to optimize the network and consequently, improve quality of life of the population.
ConclusionsThe assessment and diagnosis, selection and adaptation of hearing aids, monitoring, and speech therapy/audiology procedures offered by Hearing Health Network were performed in all regions of the state, with speech/audiological therapy and follow-up procedures representing the most and the least often performed, respectively. There was a lack of systematic spatial distribution pattern between the procedures in the health care micro-regions at the four moments of care offered to individuals with hearing impairment. Although hearing health services are available, according to the organizational policy of regionalization, the use of this network still shows very heterogeneous patterns when comparing the health micro-regions in the state.
Conflicts of interestThe authors declare no conflicts of interest.
We would like to thank Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG) for the financial support for the development of the project “Evaluation of Hearing Health Network implementation: A case study of the micro-regions of Sete Lagoas and Curvelo, Minas Gerais”, process: A PQ-03622-10, Edict: PPSUS MS/CNPq/FAPEMIG/SES 2008–2009.
Please cite this article as: de Rezende CF, Carvalho SAS, Maciel FJ, de Oliveira Neto R, Pereira DVT, Lemos SMA. Hearing health network: a spatial analysis. Braz J Otorhinolaryngol. 2015;81:232–9.


