
To verify the receiver in the ear and receiver in the aid adaptations by measuring in situ the speech perception and users’ level of satisfaction.
MethodsThe study was approved by the research ethics committee (Process: 027/2011). Twenty subjects older than 18 years with audiological diagnosis of mild and moderate bilateral descending sensorineural hearing loss were evaluated. The subjects were divided into two groups, where G1 (group 1) was fitted with open-fit hearing aids with the built-in receiver unit (receiver in the ear) and G2 (group 2) was fitted with open-fit hearing aids with RITE. A probe microphone measurement was performed to check the gain and output provided by the amplification and for assessment of speech perception with Hearing in Noise Test with and without hearing aids. After a period of six weeks of use without interruption, the subjects returned for follow-up and answered the Satisfaction with Amplification in Daily Life questionnaire, and were again subjected to Hearing in Noise Test.
ResultsBoth groups presented better test results for speech recognition in the presence of noise.
ConclusionGroups 1 and 2 were satisfied with the use of hearing aids and improved speech recognition in silent and noisy situations with hearing aids.
Estudo clínico prospectivo para verificar as adaptações RITE e RITA por meio da mensuração in situ da percepção da fala e satisfação dos usuários.
MétodoEstudo aprovado pelo CEP (Processo no 027/2011). Foram avaliados 20 indivíduos maiores de 18 anos com diagnóstico audiológico de perda auditiva sensorioneural descendente bilateral de graus leve e moderado. Os indivíduos foram divididos em dois grupos, onde o G1 (grupo 1) foi adaptado com AASI open-fit com receptor no próprio aparelho (RITA) e o G2 (grupo 2) foi adaptado com AASI open-fit com receptor no canal (RITE). Foi realizada a medida com microfone-sonda para verificação do ganho e saída do AASI e avaliação da percepção da fala com Hearing in Noise Test (HINT), sem e com AASI. Após um período de seis semanas de uso sem interrupções, o individuo retornou para acompanhamento e respondeu ao questionário SADL (Satisfaction with Amplification in Daily Life Scale) e realizou o HINT.
ResultadosOs grupos apresentaram melhores resultados no teste de reconhecimento da fala com presença de ruído.
ConclusãoOs grupos 1 e 2 apresentaram satisfação com o uso do AASI e melhora no reconhecimento de fala nas situações de silêncio e ruído com o uso de AASI.
Much has been discussed regarding the hearing aid (HA) adaptation in subjects with sloping hearing loss.1 The occlusion effect is one of their major complaints as due to the configuration of the loss, which is reported as autophonia.
Considering the technological evolution in the development of HA and the particular configuration of the hearing loss in these cases, open fit-specific mini behind-the-ear (BTE) devices provide benefits to these individuals. This model uses a shaft and a flexible adapter, and has an unique characteristic of amplification in medium and high frequencies.2,3
These devices are known as receiver in the ear (RITE) when the receiver is used into the ear canal and connected to the HA through a thin tube. Since the receiver is not located within the retroauricular device (BTE), this type of HA is particularly small and may have advantages regarding sound quality and comfort. Receiver in the aid (RITA) devices feature the receiver in the HA itself.
Both fitting and verification should be perceived as a process with a main objective: the optimum adaptation of the individual to the amplification characteristics. Researchers4 have developed a guide whereby the verification process by probe microphone measurement is part of the procedures for a proper HA fitting. The probe microphone measurement is the preferred method for verification of HA in situ.5
Probe microphone measurements can be used for checking adjustments made in the HA and to assess the efficacy of special circuits such as noise reducers, feedback reducers, directional microphones, and open-fitting HA.6–8
The main aim of the adaptation of HA is to improve speech intelligibility, thus facilitating the communication process; hence the importance of testing the individual's speech perception.9 With this investigation, it is possible to obtain the threshold of speech recognition with and without competitive noise through the Hearing in Noise Test (HINT),10 which consists of a series of 12 lists of 20 sentences with the same extension, phonetic distribution, and degree of difficulty, which were normatized so as to present a natural aspect and reliability.
During the process of counseling hearing-impaired patients, the three processes of motivation related to the use of HA should be considered: acceptance, benefit, and satisfaction.11 The success of the adaptation process of amplification depends, among other factors, on the individual's satisfaction with the results of the use of HA.12
Satisfaction is the outcome measure of auditory rehabilitation that represents the most comprehensive combination of factors needed for the final result, since the variable of interest is the point of view of the individual, and it is not related only to the performance of HA,13 but rather depends exclusively on the perceptions and attitudes of the individual.14
The measurement of satisfaction with the use of HA in daily life has also been studied using the Satisfaction With Amplification in Daily Life (SADL) questionnaire.13 This tool was designed to assess the satisfaction of HA users, quantifying it through a scoring process of four subscales: positive effects, costs and services, negative factors, and self-image.15,16
In the field of phonoaudiology, studies that critically contribute to the process of HA fitting in centers accredited by the national politics of hearing healthcare are lacking.17 The present study prioritized the evaluation of open-fitting devices using objective and subjective tools and favoring the options of RITE or RITA.
This study aimed to verify the performance of RITE and RITA adaptations by measurements in situ, speech perception, and users’ satisfaction.
MethodsThis was a prospective clinical study, conducted after approval by the Research Ethics Committee, process No. 027/2011. All participants were informed about the objectives and methodology of the proposed study, agreed to the procedures necessary for conducting the research, and signed an informed consent.
For sample composition, the following eligibility criteria were established: subjects older than 18 years with audiological diagnosis of bilateral sensorineural hearing loss at high frequencies, of mild to moderate degree, and with no prior experience with amplification.
Subjects with unilateral hearing loss or with previous experience with the use of HA; who did not continue the process of adaptation; or who did not agree to participate in the study were excluded.
The sample consisted of 20 subjects, randomly divided into two groups: group 1 (G1), users of open-fit HA adaptation with RITE, and group 2 (G2), users with conventional open-fit HA adaptation (RITA). Both groups consisted of ten subjects with similar auditory characteristics and communicative needs.
The degree of hearing loss was classified using the audiometric thresholds at 500, 1000, 2000, and 4000Hz, rated as mild (average 26–40dB NH), moderate (average 41–60dB NH), severe (average of 61–80dB NH), and profound (average above 81dB NH), according to the World Health Organization criteria.18
The participants were bilaterally fitted with a Claris-Oticon HA device, with the same criteria of prescriptive method (NAL-NL1), which has as underlying logic the loudness equalization, i.e., the formula assumes that speech intelligibility will be maximized when all frequency bands are perceived by the user as having the same loudness.
At the consultation for the adaptation procedure, a probe microphone measurement of the gain and output provided by the amplification was performed, in addition to an evaluation of speech perception with and without HA. The procedure lasted approximately 90min in this first phase of the study.
Probe microphone measurementProbe microphone measurements were performed in a sound-proof room with adequate size. The patient was positioned one meter away from the loudspeaker at 0° azimuth, using Affinity 2.0 (Interacustics) equipment.
The information related to specified acoustic characteristics with respect to the tubing type and olive size was inserted. The following measurements were performed: real ear unaided response (REUR), open-fit calibration; real ear occluded response (REOR), to verify any possible occlusion of the external auditory meatus (EAM) by the olive; and real ear aided response (REAR).
The resonance response with the use of amplification (REAR) was obtained with speech noise stimuli at 50dB SPL, 65dB SPL, and 80dB SPL intensities.
The values of REAR, at frequencies of 250, 500, 1000, 2000, 3000, 4000, and 6000Hz for input levels of 50, 65, and 80dB SPL, were compared with the NAL-NL1 rule targets for weak, medium, and strong sounds, respectively. The obtained responses were considered equivalent when the difference between the target to real ear insertion gain (REIG) and the real value obtained in ear did not exceed 10dB.19
Hearing In Noise Test (HINT)The assessment of speech perception was held by the HINT, adapted for Brazilian Portuguese,20 under four conditions:
- -
Sentences presented in silence: the HINT sentences adapted to Brazilian Portuguese were recorded at the House Ear Institute (Los Angeles, USA) by a Brazilian professional actor.
- -
Speech with front noise (FN): 20 sentences derived from a frontally positioned sound box (0°) and presented simultaneously with noise at a fixed intensity of 65dB NH in the same frontal box (0°). A composite-type noise masker was used.
- -
Speech with noise to the right (RN): 20 sentences derived from a frontally positioned box (0°) with noise presented at a fixed intensity of 65dB NH in a box to the right (90°). A composite-type noise masker was used.
- -
Speech with noise to the left (LN): 20 sentences derived from a frontally positioned box (0°), with noise presented at a fixed intensity of 65dB NH in a box to the left (90°). A composite-type noise masker was used.
The evaluation was performed without HA, with HA, and six weeks after the adaptation. The acoustically-treated room and the space allowed for the proper placement of the participant, examiner, and equipment.
After calibration of the system, the participant was instructed to remain in the same position throughout the test, ensuring that the intensity that would reach the ear would be the same as indicated on the computer screen.
For each condition, a list of 20 sentences was presented, and the list was chosen randomly by the HINT PRO software. The participants were instructed verbally, according to the guidelines contained in the HINT operating manual.
The sentence was considered correct by the examiner when all essential words were repeated correctly. In this case, the examiner pressed the ‘Yes’ button on the software screen. When ‘Yes’ was selected after the first presentation, the second sentence was presented 4dB below the intensity of the first sentence.
For the test conducted in silence, the speech level was initially set at 60dB. There was variation in intensity according to the responses of the participant – if he/she failed to correctly repeat the sentence, the level of presentation would be progressively increased by 4dB, until the participant could repeat the sentence correctly.
The scoring for the test conducted in silence, defined as the threshold of recognition of 50% of the sentences, was expressed in dB NH.
In the evaluation in presence of noise, the stimulus was presented at a fixed level of 65dB (A) and the level of speech waxed and waned according to the responses of the participant tested, until a level of 50% of speech recognition was reached.21 The score, defined as the threshold for signal-to-noise ratio after application of a list of 20 sentences, was expressed in dB. Thus, the lower the signal-to-noise ratio, the better the speech perception of the participant in this condition.
After a period of six weeks of uninterrupted use, the participant returned to the clinic for follow-up. At this stage, he/she answered the SADL questionnaire administered by the researcher, in order to verify the satisfaction level of the individual with the use of amplification. Uninterrupted use of HA was defined as the use for longer than 8h/day.
The second stage of the study, with the realization of HINT and application of SADL questionnaire, lasted for approximately 1h.
Satisfaction with Amplification in Daily Life Scale – SADLThe SADL questionnaire is an instrument designed to assess users’ satisfaction with HA. This questionnaire contains 15 questions divided into four subscales: positive effects (six items associated with acoustic and psychological benefit), services and costs (three items associated with professional competence, product price and number of repairs), negative factors (three items related to environmental noise amplification, presence of feedback and the use of telephone), and self-image (three items related to esthetic factors and to the stigma of using HA).13
Considering the 15 items of SADL, in 11 the score attributed by the participants coincided with the scoring scale, and in the other four items (questions 2, 4, 7, and 13) there was an inverse relationship between the score and the scale (i.e., in these questions the score 1 receives 7 points, expressing greater satisfaction). The higher the numerical results obtained by averaging the responses of each subscale, the greater the individual's satisfaction. Questions 1, 3, 5, 6, 9, and 10 are related to positive effects of the subscale; questions 2, 7, and 11 are related to negative factors of the subscale; questions 4, 8, and 13 are related to the subscale ‘self-image’; and questions 12, 14, and 15 refer to the subscale ‘services and costs’.14
ResultsThe results of the probe microphone measurements were defined as expected (target) responses, and as responses obtained of sound pressure level with the use of amplification (REAR), in the intensity of 50, 65, and 80dB SPL.
For groups 1 and 2, a maximum difference of 10dB was observed between the expected results and those obtained in the whole frequency range in the three input levels. No discrepancies between the results obtained at all frequencies for the whole sample were noted, and no response was obtained exceeding the expected answers, respecting the established prescription rules.
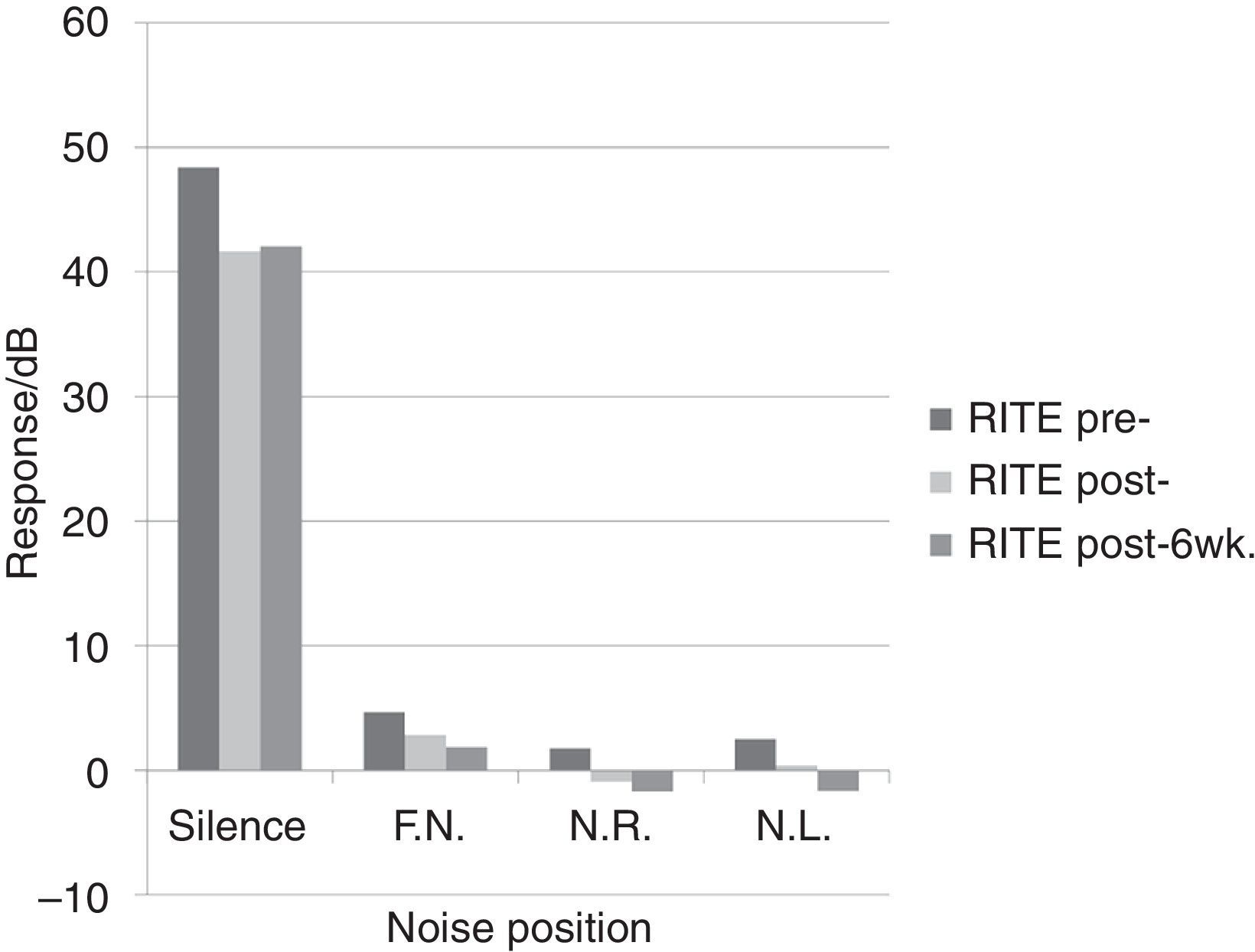
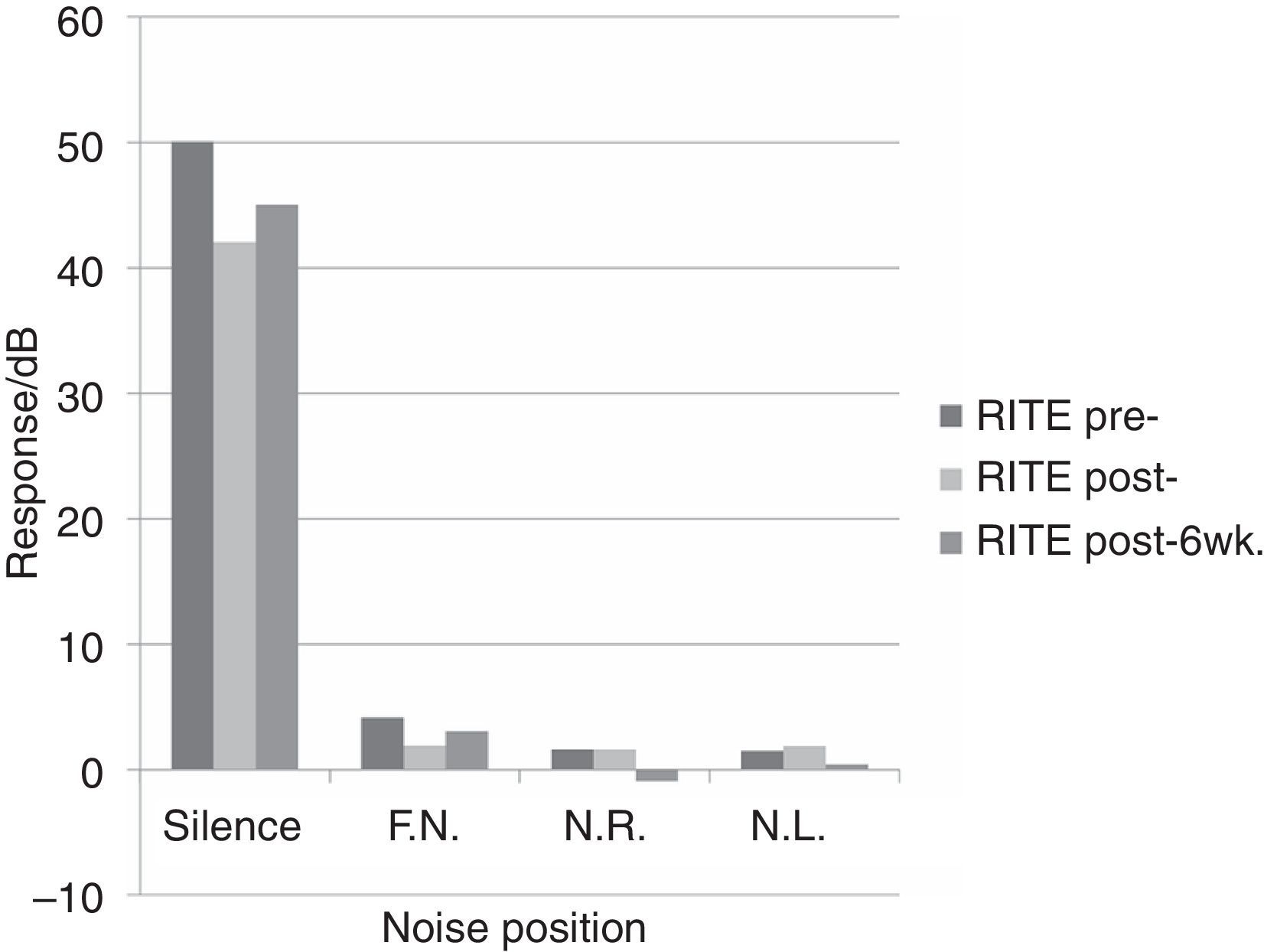
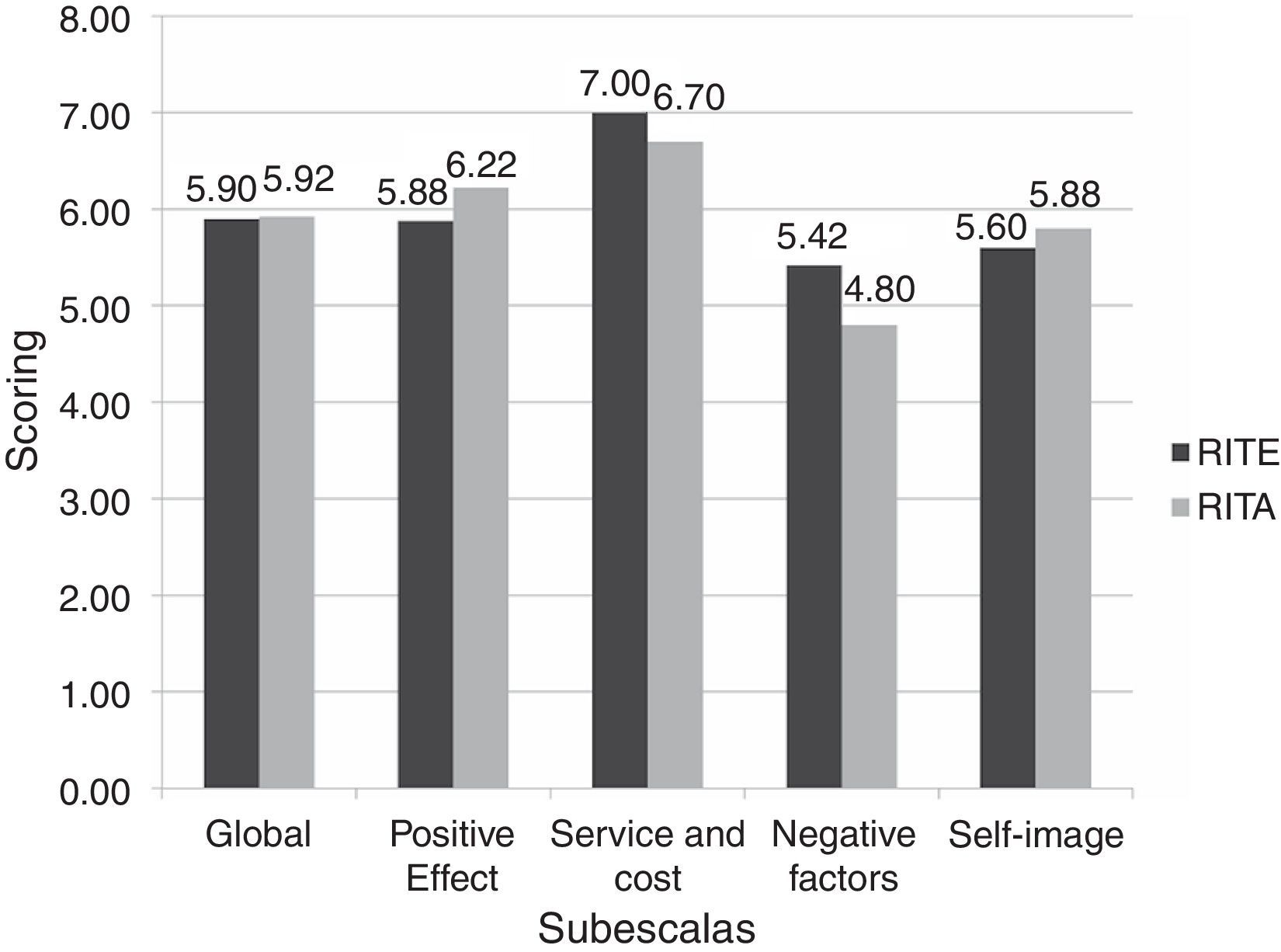
Regarding the results of HINT, Figs. 1 and 2 depict the data obtained in patients with RITE and RITA fittings, respectively. The results from SADL questionnaire are described in Fig. 3.
 at three times: without hearing aid (HA), with HA, and six weeks after the fitting (n=10).")
 at three times: without hearing aid (HA), with HA, and six weeks after the fitting (n=10).")
 and receiver in the aid (RITA) hearing aid users in the four subscales of the Satisfaction with Amplification in Daily Life (SADL) questionnaire (n=20).")
Considering the results of HINT between groups 1 and 2, analysis of variance (ANOVA) revealed a statistically significant difference (p=0.01) between the factor ‘without HA’ and ‘with HA’ in a silence condition. Evaluating such significance, the Tukey test revealed no significant difference between the groups of RITE and RITA HA users.
As for the results in the presence of noise, there was no significant difference between RITA and RITE users, regarding to the time of use of HA and to noise positioning. Fig. 1 indicates that, in the noise positions ‘in front’, ‘to the right’, and ‘to the left’, group 1 patients showed improvement in speech perception, according to the time of use of HA.
In Fig. 2, the group of RITA users showed better results in speech perception test in the presence of noise to the left and to the right, with a longer use of the HA test.
When the degree of satisfaction of participants from both groups was compared using ANOVA for two criteria, no statistically significant difference was observed in any subscale.
DiscussionThe probe microphone measures consist of an objective and accurate technique to check whether the performance of the HA in the ear of the user is equivalent to a given curve (or a set of curves) of gain or output per prescribed frequency. These measures are considered to be a good practice in the fitting procedure of these devices.4,5,8,19,22,23 In this study, these measurements were performed, suggesting that the adequacy of HA settings to the target can provide better speech recognition and, in consequence, greater users’ satisfaction with the device. The groups had their HA adjusted according to prescriptive methods, and all participants reached the target, being considered a difference of 10dB.19
Regarding the speech recognition tests, it is known that they can be used to predict the difficulties that people will have in certain environments when using HA. Furthermore, these tests facilitate the speech therapist's decision-making process regarding the need for specific training or use of other devices.19
The speech tests in noise conditions were developed in an attempt to hamper the identification of a speech signal and to simulate real-life situations experienced by patients.24 In addition, the information obtained from speech perception in noise tests can be used to accomplish the therapeutic planning for a given patient.25
In this study, the results of HINT obtained by analysis of variance (Figs. 1 and 2) indicated a statistically significant difference (p=0.01) between the responses with and without HA in condition of silence. The Tukey test revealed no significant difference between the groups of RITE and RITA HA users. This result demonstrates that HA provides a significant improvement in speech recognition in condition of silence for both groups of subjects; however, when this variable was compared after six weeks, there was no significant difference.
Regarding the results in the presence of noise, there was no significant difference between RITE and RITA users in relation to the time of use of HA and the noise position. Fig. 1 shows that in front, right, and left positions of the noise, subjects in group 1 (RITE users) showed improvement in speech perception regarding the time of HA fitting. In Fig. 2, the group of RITA users, after six weeks using the HA device, showed improvement in the speech perception test with presence of noise in front and right positions.
For both groups, when the situation without HA and after six weeks of adaptation was compared, a significant improvement in speech perception in presence of noise was observed. In a study of open-fit users, it was found that the effect of acclimatization that occurs with HA users results in improvement in the speech recognition skills, and hence in the communication and user satisfaction.26
The use of sound amplification can improve the speech recognition over time, after a period of six to 12 weeks of amplification.27 Thus, acclimatization refers to the period following the HA fitting, when a progressive improvement of listening skills and speech recognition occurs, as a result of the new clues of speech available for amplification users.28
Considering that a successful HA fitting involves multiple aspects, the benefits of acclimatization cannot be limited only to the improvement in speech recognition, but also to matters involving all aspects of the user’ communication, and that provides a level of satisfaction, thanks to his/her new condition of listener.29
Regarding the satisfaction with the use of HA (Fig. 3), the results of the SADL questionnaire subscales (positive effect, service and cost, negative factors, and self-image) were higher than the results in the normalization, with lower values13 for both groups. Only the subscale ‘self-image’ for RITE amplification users confirmed the normative data. A high level of satisfaction in the subscale ‘positive effect’ was noted for the groups – a result similar to data from a national survey.30
In general, the participants were satisfied in all subscales with the use of HA, regardless of the location of the receiver. No significant relationship between the degree of satisfaction of the participants was found, when the responses of the groups in the questionnaire as a whole were compared.
The data obtained are consistent with a study emphasizing that the experience with the audiological service/support influences on the satisfaction with HA use; subjects who reported their satisfaction with the support received also tended to report greater satisfaction with the device.31
In a study of 25 adult open-fit users, the Abbreviate Profile of Hearing Aid Benefit (APHAB) questionnaire was applied to measure the individual benefit with the different positions of the receiver, with no significant result between RITE and RITA. However, greater user satisfaction was observed with RITE, due to the appearance, comfort, retention, and speech intelligibility.32 The study in question observed similar data for both adaptations (RITE and RITA); however, the responses were significantly better, compared to the absence of amplification.
Based on the above considerations, this study demonstrated the relevance of the investigation of the benefits provided by the amplification for patients with sloping hearing loss, thus facilitating the decision-making process regarding the prescription of HA in centers accredited by the Brazilian hearing healthcare policy.
ConclusionIndividuals with sloping hearing loss using an open-fit system showed improvement in auditory performance, according to objective and subjective measurements, considering the high-level satisfaction with the use of amplification and the improvement in speech recognition in situations of silence and noise. There was no difference in performance between RITE and RITA users.
FundingThis study was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP). Process n. 2011/01454-0.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Mondelli MF, Garcia TM, Hashimoto FM, Rocha AV. Open fitting: performance verification of receiver in the ear (RITE) and receiver in the aid (RITA). Braz J Otorhinolaryngol. 2015;81:270–5.
Institution: Faculdade de Odontologia de Bauru (FOB/USP), Bauru, São Paulo, SP, Brazil.
gology tem o prazer em homenagear os revisores


