

Auditory steady-state responses (ASSR) are an important tool to detect objectively frequency-specific hearing thresholds. Pure-tone audiometry is the gold-standard for hearing evaluation, although sometimes it may be inconclusive, especially in children and uncooperative adults.
AimCompare pure tone thresholds (PT) with ASSR thresholds in normal hearing subjects.
Materials and methodsIn this prospective cross-sectional study we included 26 adults (n = 52 ears) of both genders, without any hearing complaints or otologic diseases and normal pure-tone thresholds. All subjects had clinical history, otomicroscopy, audiometry and immitance measurements. This evaluation was followed by the ASSR test. The mean pure-tone and ASSR thresholds for each frequency were calculated.
ResultsThe mean difference between PT and ASSR thresholdswas 7,12 for 500Hz, 7,6 for 1000Hz, 8,27 for 2000Hz and 9,71dB for 4000Hz. There were no difference between PT and ASSR means at either frequency.
ConclusionASSR thresholds were comparable to pure-tone thresholds in normal hearing adults. Nevertheless it should not be used as the only method of hearing evaluation.
© 2014 Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial. Published by Elsevier Editora Ltda. All rights reserved.
As respostas auditivas de estado estável permitem avaliar de forma objetiva limiares auditivos frequência-específica. A audiometria tonal é o exame padrão-ouro; no entanto, nem sempre pode ser conclusiva, principalmente em crianças e adultos não colaborativos.
ObjetivoComparar os limiares auditivos da RAEE aos da audiometria tonal em indivíduos com audição normal.
Materiais e métodosForam incluídos neste estudo prospectivo de corte transversal 26 adultos (52 orelhas), de ambos os gêneros, com audiometria normal e sem queixas otológicas. Os pacientes foram submetidos a anamnese, otomicroscopia, audiometria e imitanciometria. A seguir, realizou-se avaliação de respostas auditivas de estado estável. Os resultados obtidos foram analisados estatisticamente e comparados entre si.
ResultadosA diferença entre os limiares (em dB NA) obtidos em ambos os exames para cada frequência testada foi de 7,12dB para 500Hz; 7,6dB para 1000Hz; 8,27dB para 2000Hz e 9,71dB para 4000Hz, com limiares mais elevados na RAEE, em todas as frequências. Não houve diferença estatística entre as médias para cada frequência testada.
ConclusãoOs limiares obtidos na RAEE foram comparáveis aos da audiometria tonal em indivíduos normouvintes; entretanto, não deve ser usado como único método de avaliação auditiva.
© 2014 Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial. Publicado por Elsevier Editora Ltda. Todos os direitos reservados.
Auditory steady-state responses (ASSR) assessment has an important place in the arsenal of audiological evaluation methods. Since the introduction of universal neonatal hearing loss has been diagnosed earlier, and thus arises the need to define the characteristics of hearing loss in order to choose the most appropriate treatment.1-3
Due to limitations of the responses obtained in behavioral tests in children younger than 6 months, electrophysiological methods are the most used resources.
The tone-burst evoked potential is the preferred test for frequency-specific assessment in childhood, which provides the electrophysiological threshold for each frequency tested. The limitations of this procedure are time, since the test is usually long, and the difficulty and subjectivity in the interpretation of the responses. Nevertheless, the assessment of evoked potentials with transient stimuli such as tone bursts does not allow for stimulation at levels greater than 90dB HL.4
In adults, pure-tone (PT) audiometry is the gold standard for obtaining thresholds and audiometric configuration. However, this test is subjective and it is not always possible to perform in children younger than 6 years of age, especially when some psychomotor impairment is present.
The increasingly more frequent use of ASSR is due to the possibility of objectively evaluating the electrophysiological thresholds in patients with suspected hearing impairment. For that purpose, it would be appropriate to perform a comparative study with other already established methods and ASSR. According to John and Picton,5 and Valdes et al.,6 the method has advantages, such as the objective threshold detection as well as the simultaneous evaluation of multiple frequencies7 and the presentation of high intense stimuli.8
Since ASSR allows for the assessment of different frequencies in both ears at the same time, the duration of the examination is usually shorter.9 As there are different ASSR equipments and software, and a higher difference between PT and ASSR thresholds in the low frequency may occur, the results should be interpreted with caution.10-12
Among the software with large number of studies in the literature, Audera and Multiple Auditory Steady-State Response (MASTER) must be highlighted. The Audera is based on single frequency stimulation, is usually monaural, and uses phase coherence as a response detection method.13 The MASTER software allows for simultaneous binaural stimulation, with continuous tones at four frequencies (500, 1,000, 2,000, and 4,000Hz) modulated in amplitude and frequency. It is believed that the responses generated in frequency modulation between 70 and 110Hz reflect the activity of the auditory brainstem structures.14
Responses are converted from their original form in the time domain to the frequency domain by fast Fourier transform (FFT). They appear as peaks in the modulation frequency domain, which emerge from electroencephalogram (EEG).15 They are then evaluated against background noise, and statistical significance is determined by the software itself (MASTER) through the F-test.16,17
The results are shown as an electrophysiological audiogram, which allows the physician to see the configuration of hearing loss, if any, and make the appropriate choice of treatment (amplification, cochlear implant, or others).
Several studies have determined the reliability of evaluating the objective threshold in individuals with normal hearing or sensorineural hearing loss.18-20 Most of them aimed to compare PT audiometry with ASSR, analyzing patients with varying degrees of hearing loss together with normal hearing individuals. Lins et al.10 evaluated 117 patients, including adults with and without hearing loss, adolescents, and children. Canale et al.21 included 11 patients, six of whom with normal hearing and five with hearing loss. Valdes et al.6 studied 15 patients with normal hearing; however, they only evaluated the frequencies of 500 and 1,000Hz. As for Brazilian authors, Ferraz et al.22 studied 25 individuals with no hearing complaints, whereas Duarte et al.23 evaluated 48 patients with varying types of hearing loss.
The small number of publications at the Brazilian level and the need for standardization of thresholds in normal hearing subjects for clinical practice was the rationale for this study in this population. The MASTER software was chosen, as it allows for binaural stimulation of four frequencies simultaneously.
This study aimed to compare the electrophysiological thresholds obtained by ASSR with those obtained by PT audiometry in normal hearing adults.
Materials and methodsParticipantsA total of 28 normal hearing adults (n = 56 ears), of both genders, between 18 and 35 years were evaluated in this cross-sectional study. The study was performed between July and December of 2011. All participants were informed of the study purpose and signed the informed consent. The study was approved by the ethics committee of the institution under number 0058/11.
The individuals were selected according to the following inclusion criteria: no ear or hearing complaints; normal otomicroscopy; normal PT audiometry; with thresholds ≤ 25dB HL at frequencies of 250, 500, 1,000, 2,000, 3,000, 4,000, 6,000 and 8,000Hz; normal immitance, i.e., type A tympanometry; and present stapedial reflexes. The study excluded individuals with any morphological and functional alterations of the external or middle ear, detected at the anamnesis or otorhinolaryngological examination, as well as those who had any of the above mentioned hearing disorders or neurological alterations. Those who did not reach an appropriate level of electroencephalographic noise for response recording (< 30μν) were also excluded.
Audiological assessmentAnamnesis and otorhinolaryngological clinical examinationAll patients underwent otorhinolaryngological clinical examination directed at hearing complaints. Then all patients were submitted to otomicroscopy (model M9000 - DF Vasconcellos - Valença, RJ, Brazil).
Audiometry and immitanciometryPT audiometry was performed in a sound booth using a Madsen Midimate 622 audiometer (GN Otometrics - Copenhagen, Denmark) calibrated according to American National Standards Institute (ANSI) S3.6-1996 standards. Tone thresholds by air conduction were obtained with PT at frequencies of 500, 1,000, 2,000, and 4,000Hz presented through supra-aural headphones (TDH 39)
For tympanometry and stapedial reflex measurements at 500, 1,000, 2,000, and 4,000Hz, an AZ26 Interacoustics impedanciometer (Interacoustics A/S - Assens, Denmark) was used.
Stimuli and auditory steady-state response acquisitionBio-Logic Navigator Pro 580 NAVPR2 equipment (Natus Medical Incorporated - San Carlos, CA, USA) and the MASTER 2.04.i00 software were used. Stimuli by air conduction were calibrated in dB NPS, according to the ANSI S3.6-1996 standard, using a Quest Model 1700 sound level meter with a 2cm3 Brüel & Kjær DB138 coupler.
The disk electrodes were placed on the frontal region (Fz) as the active electrode, neck (Oz) as reference, and right shoulder as ground (Pz). Eight simultaneous stimuli of modulated continuous tones (100% modulation in exponential amplitude and 20% in frequency) were offered, following the procedure pre-established by the manufacturer, starting at 40dB HL. Modulation rates for the right ear were 84.375Hz, 89.062Hz, 93,750Hz and 98,437Hz for 500, 1,000, 2,000, and 4,000Hz, respectively, and for the left ear, 82.031Hz, 86.719Hz, 91.406Hz and 96.094Hz for 500, 1,000, 2,000, and 4,000Hz, respectively. The maximum number of sweeps (32 sweeps at the intensities of 40dB HL and 30dB HL and 40 scans at lower intensities down to threshold) were performed following the manufacturer’s recommendation to ensure better test reliability.
The threshold was established by modifying the intensity level by 5dB HL, the same procedure used in audiometry. All ASSR thresholds were retested. Sweeps containing electrophysiological activity > 90nV were eliminated.17,18,24
The significance of the signal-to-noise ratio was verified by the F-test with a 95% confidence interval for each sweep. The response was considered present when the F-value was significant at the level of p < 0.05 in at least eight consecutive sweeps.25
Statistical analysisThe mean threshold obtained by PT audiometry and auditory steady state response (ASSR) was compared at 500, 1,000, 2,000, and 4,000Hz.
The descriptive analysis of the thresholds in PT audiometry and ASSR were performed by calculating central tendency measures (such as means), and measures of dispersion (such as the standard deviation [SD] and standard error) for each frequency in both methods, considering a normal data distribution.
The difference between the means at 500, 1,000, 2,000, and 4,000Hz was calculated by analysis of variance (ANOVA). The same test was used to assess the threshold differences between males and females, as well as between right and left ears (p < 0.05).
ResultsAmong the 28 initially recruited subjects (n = 56 ears), two were excluded as they failed to reach sufficient relaxation to a noise level < 30μV
The study encompassed 17 females and 9 males. There was no significant difference between genders (p = 0.82).
Among the 26 subjects, measurable thresholds were obtained in 100% of the tested frequencies in ASSR.
The age of the evaluated subjects ranged from 22 to 31 years (mean: 27.3years; SD: 2.26years).
The separate analysis of the right and left ears showed no difference in thresholds between them (p = 0.34). For further analyses, all ears were analysed together.
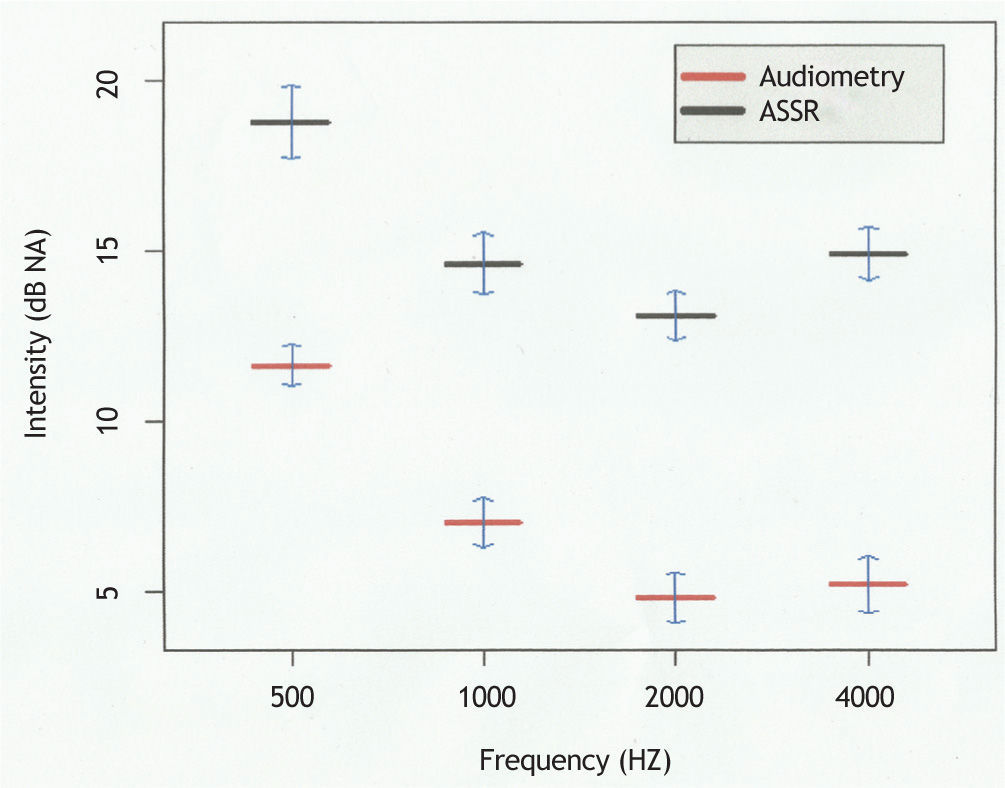
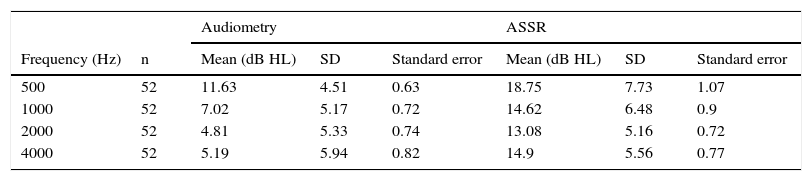
Table 1 presents the mean, standard deviation, and standard error of audiometric thresholds and steady-state responses separated by frequency.
Mean audiometric thresholds and steady-state responses (n = 52 ears) for each frequency with standard deviation (SD) and standard error.
| Frequency (Hz) | n | Audiometry | ASSR | ||||
|---|---|---|---|---|---|---|---|
| Mean (dB HL) | SD | Standard error | Mean (dB HL) | SD | Standard error | ||
| 500 | 52 | 11.63 | 4.51 | 0.63 | 18.75 | 7.73 | 1.07 |
| 1000 | 52 | 7.02 | 5.17 | 0.72 | 14.62 | 6.48 | 0.9 |
| 2000 | 52 | 4.81 | 5.33 | 0.74 | 13.08 | 5.16 | 0.72 |
| 4000 | 52 | 5.19 | 5.94 | 0.82 | 14.9 | 5.56 | 0.77 |
Fig. 1 shows the association between the thresholds obtained in the two aforementioned examinations. Thresholds obtained in the steady-state responses were consistently higher. The mean difference between the thresholds in both tests was 8.175dB, which remained constant at all frequencies (p = 0.30), i.e., there was no variability between the frequencies investigated by the two methods (Table 2).
 at frequencies of 500, 1,000, 2,000, and 4,000Hz with their respective standard error (n = 52 ears).")
Several authors6,10,18,23,25-27 have reported better correlation of PT thresholds and steady-state responses in patients with sensorineural hearing loss as compared to those with normal hearing. It has been suggested that this difference may reflect an increase in the amplitude of response due to the presence of recruitment.21,28
In 2012, Korczak et al.29 reported that there is no difference between ASSR and PT thresholds in individuals with sensorineural hearing loss compared with those with normal hearing, both in the stimulation of a single frequency and with multiple simultaneous frequencies.
In the present study, a difference of 7.12, 7.6, 8.27, and 9.71dB was observed at frequencies of 500, 1,000, 2,000, and 4,000Hz, respectively, reaching a mean difference of 8.175dB HL between audiometric and electrophysiological thresholds. There was no statistical difference between the values obtained at the assessed frequencies (p = 0.30).
In 2006, Canale et al.21 reported a mean difference of audiometric and ASSR thresholds in individuals with normal hearing of 32dB, while Ferraz et al.22 reported a mean difference of 20dB. Other authors6,29 observed results with a smaller mean difference between tests, but always above 10dB.
Some studies8,19,26,27,30 have found major differences in the frequencies of 500 and 4,000Hz, differing from the present study, in which there was no significant difference between the thresholds of the four frequencies. One reason for this finding is possibly sample homogeneity, comprising only individuals with normal hearing and age 22 to 31 years.
The smaller difference between the thresholds obtained in both tests shown in this study when compared to the literature is probably due to sample size (larger than most reported in the literature) and the adequate test conditions, especcially low background noise, allowing the identification of responses at very low intensities, which usually have a small amplitude. The test was completed after averaging 32 scans at intensities of 40dB HL and 30dB HL and 40 sweeps at lower intensities (maximum sweep number suggested by the software) for each intensity, approaching electrophysiological to PT thresholds. As the threshold was assessed at 5dB intervals, the same procedure used for PT audiometry, an increase in accuracy and decrease in variability of values was obtained.
It is important to highlight that similar results may not be obtained in clinical practice. It is not always suitable to estimate ASSR thresholds at 5dB intervals, as it can greatly increase the test time without adding data which may modify the decision on the best therapeutic approach.31 Varied age ranges (including elderly and children), levels of relaxation in awake patients, or EEG changes during sedation/anesthesia may also interfere in the threshold evaluation.
As electrophysiological thresholds are approximately 10dB HL above the tonal thresholds, the software provides a correction factor. Its use, as suggested by the software Master Bio-Logic Navigator Pro 580 NAVPR2 (Mundelein, Il) of 10dB for frequencies tested, brings the ASSR results even closer to those obtained by the audiometry.
Although this study is one of the largest exclusively normal hearing individuals, further studies with larger numbers of participants or multicenter studies are needed in order to confirm these results, especially in the Brazilian population.
These thresholds, obtained with modulated continuous-tone stimuli using the MASTER software, should not be extrapolated to represent those acquired from other available equipment that evoke ASSR with different types of stimuli (e.g. Chirp) and other methods of response detection. Further studies are needed in order to evaluate different methods of ASSR stimulation and detection to assess whether the thresholds are comparable, thus providing greater accuracy for the physician when estimating hearing thresholds.
ConclusionThe ASSR thresholds were comparable to those of tonal audiometry in individuals with normal hearing, and they showed a mean difference that remained constant at all tested frequencies. However, as electrophysiological tests only estimate hearing thresholds, the ASSR should not be used as the sole method of auditory assessment.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Beck RM, Ramos BF, Grasel SS, Ramos HF, Moraes MF, Almeida ER, et al. Comparative study between pure tone audiometry and auditory steady-state responses in normal hearing subjects. Braz J Otorhinolaryngol. 2014;80:35-40.


