
Benign fibrous histiocytoma is a condition first described by Stout1 in 1967. It often affects sun-exposed skin, but may be found in other organs, including intraosseous sites.2 In these cases, the clinical manifestations are pain and enlargement of the affected bone.
We are reporting the case of a benign mastoid fibrous histiocytoma involving the left mastoid for two years that was pathologically the same as a tumor the patient had experienced 15 years earlier in the right ear.
In the medical literature, this tumor is rarely described involving the mastoid, and we could not find any report with bilateral involvement occurring at different times.
Case presentationA 56-year-old female patient presented with a one-month history of left retroauricular pain radiating to the ipsilateral head and face. She also had left mastoid tenderness, with normal otoscopic findings and and hearing bilaterally. In addition, she reported having an operation to remove a tumor from the opposite ear 15 years earlier that was diagnosed a benign fibrous histiocytoma.
Computed tomography showed evidence of a right mastoidectomy and a lytic lesion with soft-tissue density material in the left mastoid cavity. Both middle ears were normal.
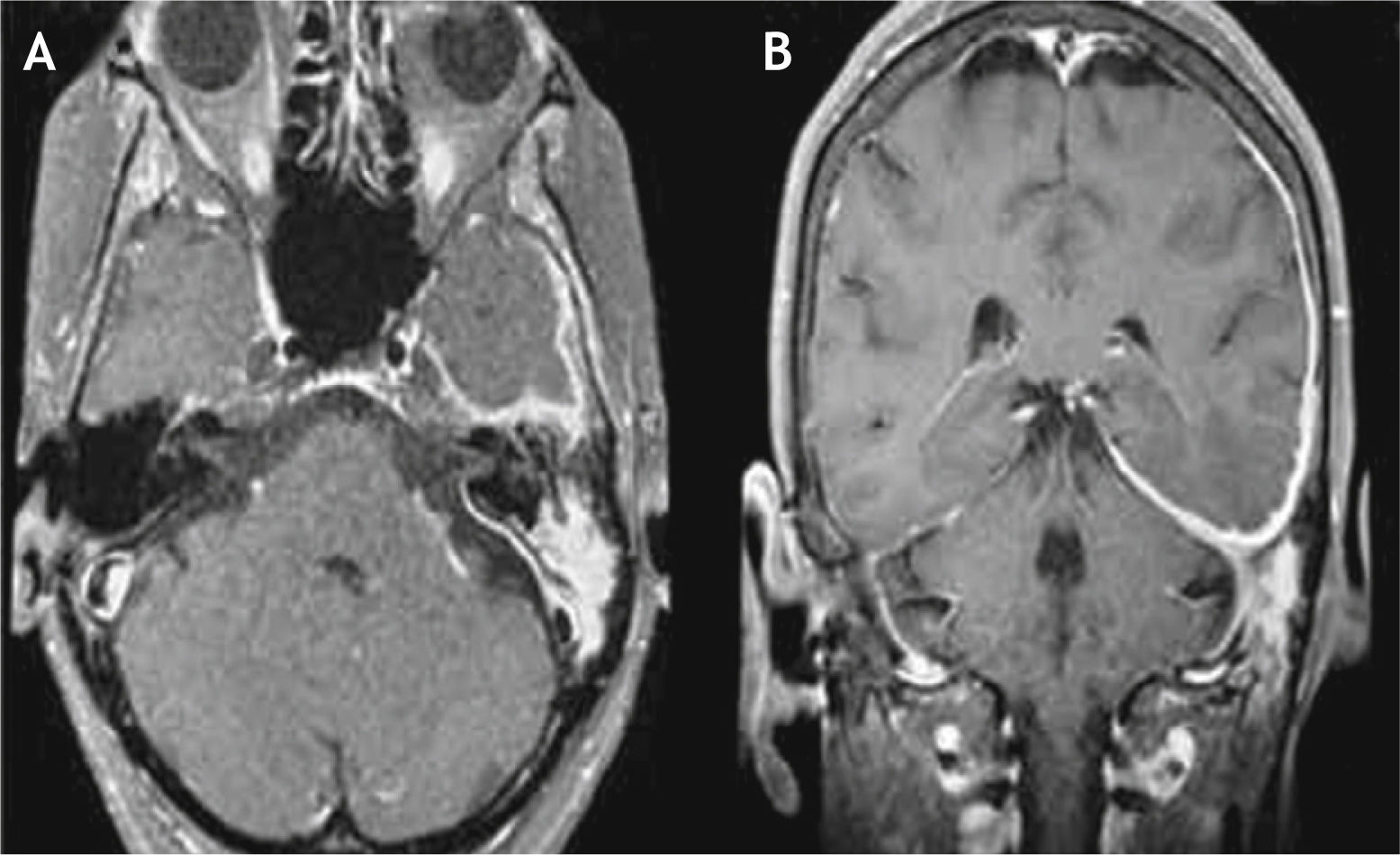
Magnetic resonance imaging showed high T2 signal seen in the left mastoid cells, with gadolinium-enhanced meningeal thickenings at the cerebellar tentorium and the ipsilateral middle cranial fossa (Fig. 1).

The patient underwent left mastoidectomy, with removal of the posterior wall of the ear canal. The lesion was confined to the mastoid cavity and did not involve the tympanic membrane, the middle ear, or the mastoid tegmen. Histological study confirmed the diagnosis of a benign fibrous histiocytoma.
The surgical cavity healed completely within three months, but the patient reported worsening headache and facial pain in the left upper dental arch. She was referred to the pain group for medical treatment, but became symptom-free only two years after the surgery.
DiscussionThe fibrous histiocytoma is a rare condition found over a large age range, between 5 and 75 years. It comprises about 1% of all bone tumors,3 often is seen in lower limb bones and is predisposed to relapses.4 Few reports describe temporal bone involvement and most of them report malignant tumors. Differential diagnostic conditions include acute inflammation, benign tumors (giant cell tumor and ossifying fibroma) and malignant lesions (fibrosarcoma and osteosarcoma). Magnetic resonance imaging excluded the possibility of inflammation since the tumor was solid. The imaging revealed extensive pachymeningitis, meningeal thickening, which was likely inflammatory in nature, and located in the paratrigeminal area. Although the surgery had removed the lesion, the contiguous bone and meningeal involvement could explain the headache and earache reported by the patient postoperatively, since no communication with the middle cranial fossa has been detected.5,6 This involvement can also explain the relapse of these tumors, making it difficult to be certain of a cure and indicating that long-term follow-up is needed. As this is a rare condition, relapse rates are variable and difficult to determine.
No involvement similar to that shown in this report was found in the literature, with bilateral involvement of temporal bones, meningeal extension, similar histological features, and development of the second tumor long after the initial lesion.
Final commentsAlthough the benign temporal bone histiocytoma is rare, this condition can be found and should be remembered in the differential diagnosis of ear tumors.
Clinical and radiological characteristics should draw the physician's attention to a careful work-up, even in bilateral cases, as in this report.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Granato L, Próspero JD, Sanvito WL, Costa LBA, Fernandes AMF. Benign fibrous histiocytoma of the temporal bone: involvement of both mastoids at different times. Braz J Otorhinolaryngol. 2014;80:264-5.


