
Tinnitus is a frequent symptom in cochlear implant patients, often reported as persistent and disabling in implant candidates. Tinnitus is rarely considered in the preoperative evaluation of patients who are eligible for cochlear implantation. Many studies have shown that a cochlear implant leads to a significant change in the perception of tinnitus.
ObjectiveTo identify evidence in the scientific literature indicating that cochlear implant in eligible patients with tinnitus can improve tinnitus perception.
MethodsOne hundred forty articles were found from nine databases, and 20 articles from the gray literature mentioned the relationship between cochlear implant and tinnitus perception in patients eligible for cochlear implant. The PICOS (population, intervention, comparison, and outcome) strategy, was used to define the eligibility criteria. The studies that met the inclusion criteria for this second step were included in a qualitative synthesis, and each type of study was analyzed using the Joanna Briggs Institute critical appraisal checklist for quasi-experimental studies and the Joanna Briggs Institute critical appraisal checklist for randomized clinical trials.
ResultsThe full texts of 11 articles were read, and 6 studies were selected for the meta-analysis. The total sample size in the evaluated articles was 136 patients with tinnitus who were eligible for cochlear implantation.
ConclusionsTaken together, these findings support the feasibility of cochlear implantation to reduce the perception of tinnitus, thus providing a new perspective in the treatment of tinnitus in patients with hearing loss who are candidates for cochlear implantation.
Tinnitus is a sensation that chronically affects approximately 4% of the general population.1 It is a frequent symptom in cochlear implant (CI) candidates, with a prevalence ranging from 66% to 86%.2 Tinnitus is often a persistent and disabling symptom in patients eligible for cochlear implantation, but it rarely receives attention in the preoperative assessment of these patients.3
A common question among candidates for cochlear implants is whether there will be any improvement in tinnitus after the procedure. There are, however, no consistent data in the literature that give us the possibility to answer this question.
Cochlear implantation has become the standard treatment for patients with severe-to-profound bilateral hearing loss who no longer derive benefit from hearing aids.4,5 Some studies describe a suppressive effect of CI on tinnitus.6
The study of how tinnitus perception changes following electrode insertion into the cochlea and cochlear implant activation can provide new insights into the pathogenic mechanisms and treatment of tinnitus.3
This study aims to evaluate the changes in tinnitus perception among patients who undergo cochlear implantation.
MethodsLiterature searchA vast literature review was performed using the PUBMED, MEDLINE, LILACS, LIVIVO, CUMED, IBECS, SPEECHBITE, GOOGLE Scholar, and Cochrane databases. The search strategy used the following terms to identify original articles and reviews published from database inception until January 2019: Cochlear implant, or cochlear prosthesis, or cochlear prosthetic devices, or cochlear prosthesis, or prosthesis, or auditory prosthesis, or CI, or implant, or “cochlear implants”, or “cochlear implantation” (Mesh terms) and tinnitus, or tinnit, or booming, or buzzing, or ringing, or tinnitus (Mesh terms). Only papers published in English were used. The strategy followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines, 7 and the protocol was registered at the international prospective register of systematic reviews–PROSPERO 8 under registration number CRD42018105930.
The references of each database were exported to the EndNote X7 program (https://endnote.com/), and then, these same references were exported from EndNote X7 to the Rayyan QCRI program (https://rayyan.qcri.org/) to increase the reliability of the selection of articles before proceeding to the eligibility stage.
Data extractionAfter identifying articles appropriate for analysis using the PICOS strategy (population, intervention, comparison, outcomes) to define the eligibility criteria, the full texts of articles were then reviewed by three blinded reviewers to identify individual patients with tinnitus before or after cochlear implantation.
The inclusion criteria were patients with moderate, severe, or profound unilateral or bilateral hearing loss with tinnitus before cochlear implantation who had their tinnitus severity measured by the tinnitus handicap inventory (THI). The THI is an internationally validated, 25-question tinnitus scoring system assessing the impact of tinnitus on the patient's psychological functioning and activities of daily life. Exclusion criteria included studies with no intervention, studies that did not evaluate tinnitus, studies with patients who were not candidates for cochlear implantation, studies with abstention from postoperative data and nonclinical studies.
After the study evaluations, the selected studies were subjected to a meta-analysis. This analysis combines and summarizes results from multiple studies, thus increasing the accuracy and the power of evidence of the results.9
For the meta-analysis, a mixed effects approach was used to detect mean differences at a 95% confidence interval for each continuous outcome. The weighted mean difference (WMD) was calculated. The statistical significance of the mean difference was evaluated using a Z-test. The heterogeneity (W2) of effect sizes was calculated using Cochrane's I2 (I2=25% indicates mild heterogeneity, 50% indicates moderate heterogeneity, and 75% indicates marked heterogeneity). Meta-analysis was performed using review manager (RevMan, version 5.2) from the Cochrane collaboration.10–12
After meta-analysis, a systematic review was conducted to analyze the questionnaires used to assess tinnitus perception.
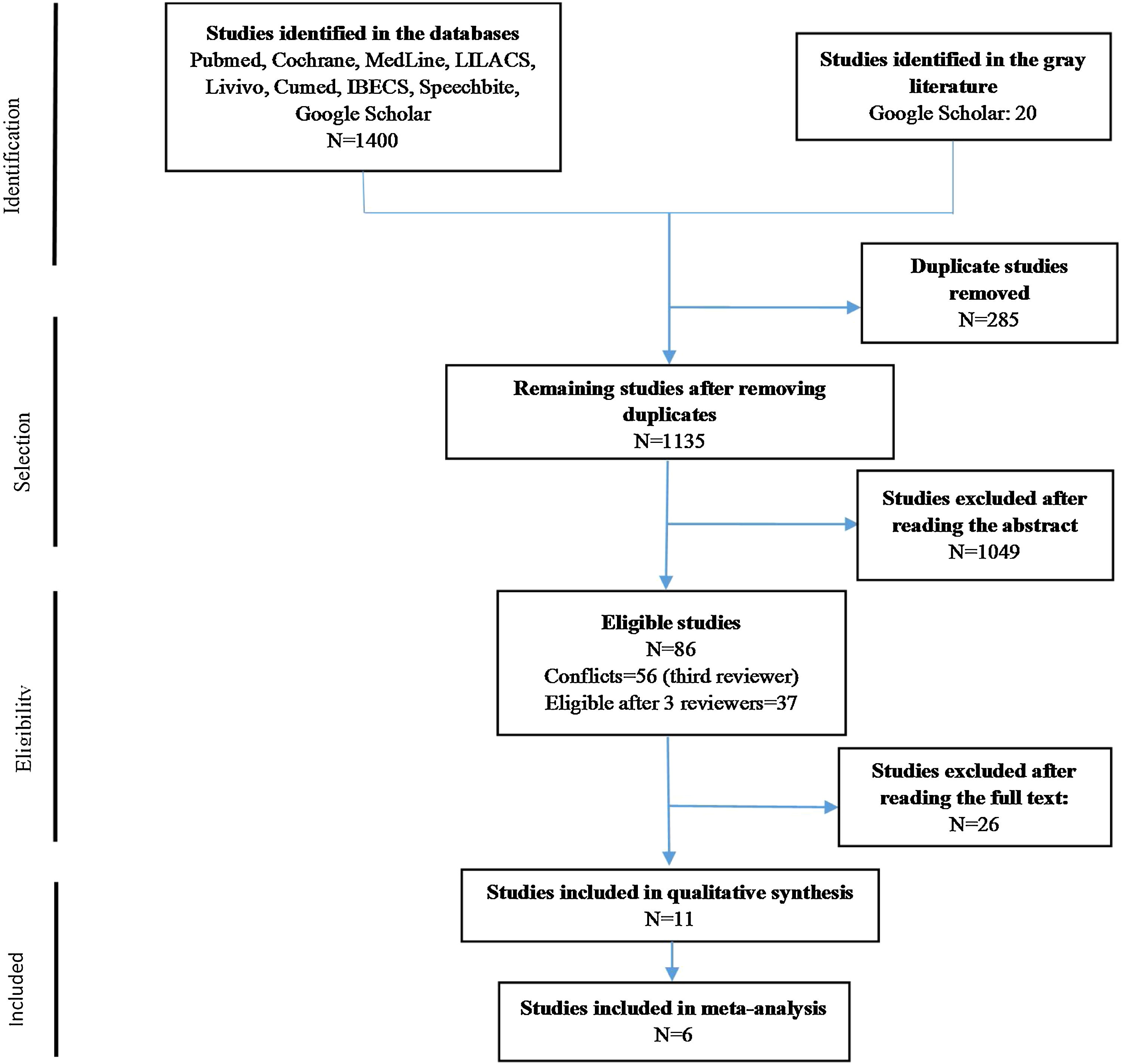
ResultsThe whole process of article selection is described in Fig. 1, which shows the flow diagram for inclusion in accordance with the PRISMA guidelines. No additional studies were found by performing a search of the reference lists of the included articles.

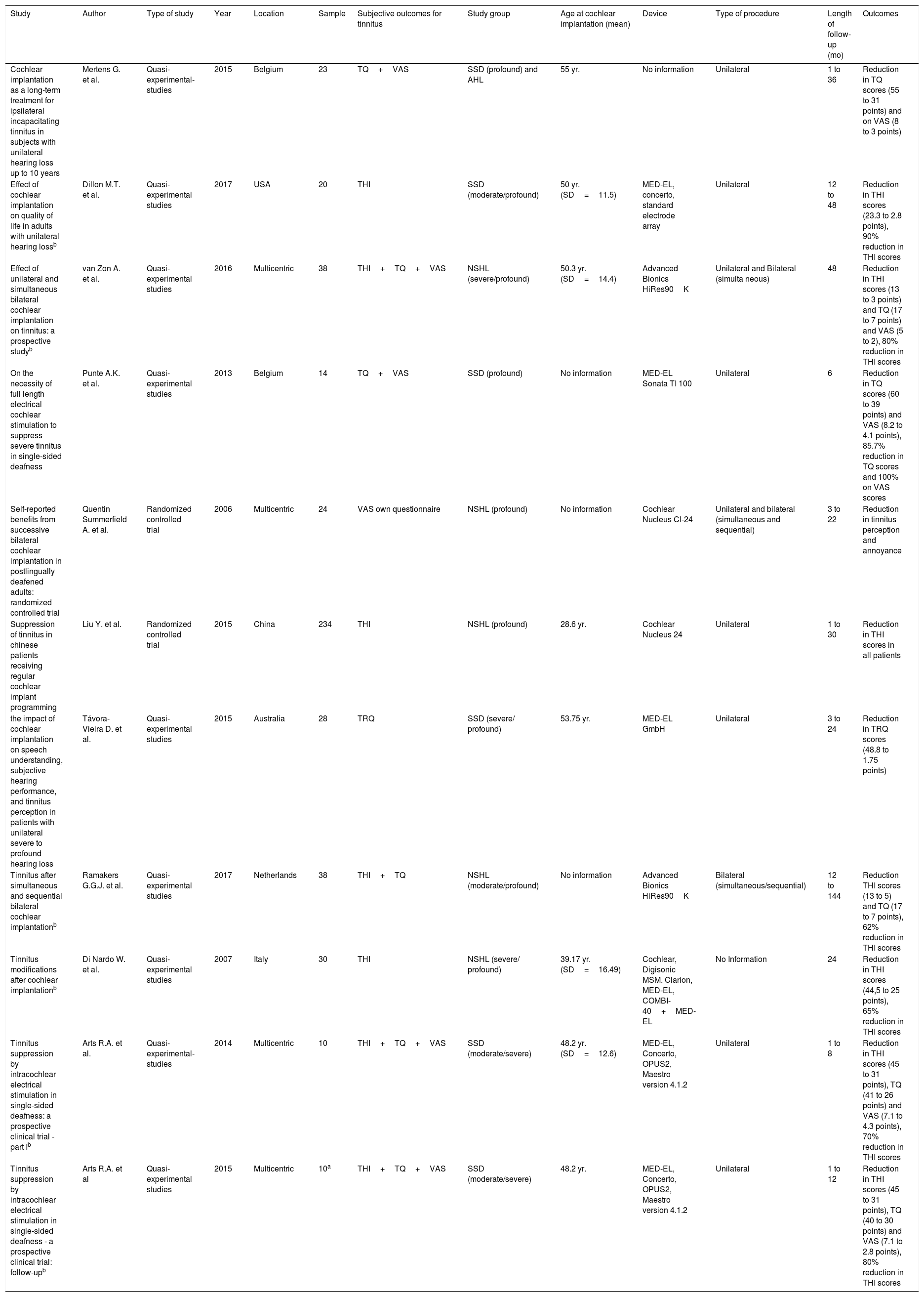
The literature review produced 11 studies for systematic review and 6 studies 3,6,13–16 suitable for meta-analysis (Table 1). The studies eligible for meta-analysis included 136 patients meeting the individual patient inclusion criteria for changes in tinnitus perception after surgery. Two papers 15,16 analyzed the same patients in a part I trial and follow-up; therefore, the 10 patients evaluated were included in the meta-analysis twice. One study rated patients in two groups, i.e., after simultaneous CI and after sequential CI; these patients were analyzed as two separate groups.14 Each study applied the THI at different timepoints (Table 1), thus providing a global idea of tinnitus perception behavior after CI.
Studies with patients meeting the inclusion criteria for meta-analysis.
| Study | Author | Type of study | Year | Location | Sample | Subjective outcomes for tinnitus | Study group | Age at cochlear implantation (mean) | Device | Type of procedure | Length of follow-up (mo) | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cochlear implantation as a long-term treatment for ipsilateral incapacitating tinnitus in subjects with unilateral hearing loss up to 10 years | Mertens G. et al. | Quasi-experimental-studies | 2015 | Belgium | 23 | TQ+VAS | SSD (profound) and AHL | 55 yr. | No information | Unilateral | 1 to 36 | Reduction in TQ scores (55 to 31 points) and on VAS (8 to 3 points) |
| Effect of cochlear implantation on quality of life in adults with unilateral hearing lossb | Dillon M.T. et al. | Quasi-experimental studies | 2017 | USA | 20 | THI | SSD (moderate/profound) | 50 yr. (SD=11.5) | MED-EL, concerto, standard electrode array | Unilateral | 12 to 48 | Reduction in THI scores (23.3 to 2.8 points), 90% reduction in THI scores |
| Effect of unilateral and simultaneous bilateral cochlear implantation on tinnitus: a prospective studyb | van Zon A. et al. | Quasi-experimental studies | 2016 | Multicentric | 38 | THI+TQ+VAS | NSHL (severe/profound) | 50.3 yr. (SD=14.4) | Advanced Bionics HiRes90K | Unilateral and Bilateral (simulta neous) | 48 | Reduction in THI scores (13 to 3 points) and TQ (17 to 7 points) and VAS (5 to 2), 80% reduction in THI scores |
| On the necessity of full length electrical cochlear stimulation to suppress severe tinnitus in single-sided deafness | Punte A.K. et al. | Quasi-experimental studies | 2013 | Belgium | 14 | TQ+VAS | SSD (profound) | No information | MED-EL Sonata TI 100 | Unilateral | 6 | Reduction in TQ scores (60 to 39 points) and VAS (8.2 to 4.1 points), 85.7% reduction in TQ scores and 100% on VAS scores |
| Self-reported benefits from successive bilateral cochlear implantation in postlingually deafened adults: randomized controlled trial | Quentin Summerfield A. et al. | Randomized controlled trial | 2006 | Multicentric | 24 | VAS own questionnaire | NSHL (profound) | No information | Cochlear Nucleus CI-24 | Unilateral and bilateral (simultaneous and sequential) | 3 to 22 | Reduction in tinnitus perception and annoyance |
| Suppression of tinnitus in chinese patients receiving regular cochlear implant programming | Liu Y. et al. | Randomized controlled trial | 2015 | China | 234 | THI | NSHL (profound) | 28.6 yr. | Cochlear Nucleus 24 | Unilateral | 1 to 30 | Reduction in THI scores in all patients |
| the impact of cochlear implantation on speech understanding, subjective hearing performance, and tinnitus perception in patients with unilateral severe to profound hearing loss | Távora-Vieira D. et al. | Quasi-experimental studies | 2015 | Australia | 28 | TRQ | SSD (severe/ profound) | 53.75 yr. | MED-EL GmbH | Unilateral | 3 to 24 | Reduction in TRQ scores (48.8 to 1.75 points) |
| Tinnitus after simultaneous and sequential bilateral cochlear implantationb | Ramakers G.G.J. et al. | Quasi-experimental studies | 2017 | Netherlands | 38 | THI+TQ | NSHL (moderate/profound) | No information | Advanced Bionics HiRes90K | Bilateral (simultaneous/sequential) | 12 to 144 | Reduction THI scores (13 to 5) and TQ (17 to 7 points), 62% reduction in THI scores |
| Tinnitus modifications after cochlear implantationb | Di Nardo W. et al. | Quasi-experimental studies | 2007 | Italy | 30 | THI | NSHL (severe/ profound) | 39.17 yr. (SD=16.49) | Cochlear, Digisonic MSM, Clarion, MED-EL, COMBI-40+MED-EL | No Information | 24 | Reduction in THI scores (44,5 to 25 points), 65% reduction in THI scores |
| Tinnitus suppression by intracochlear electrical stimulation in single-sided deafness: a prospective clinical trial - part Ib | Arts R.A. et al. | Quasi-experimental-studies | 2014 | Multicentric | 10 | THI+TQ+VAS | SSD (moderate/severe) | 48.2 yr. (SD=12.6) | MED-EL, Concerto, OPUS2, Maestro version 4.1.2 | Unilateral | 1 to 8 | Reduction in THI scores (45 to 31 points), TQ (41 to 26 points) and VAS (7.1 to 4.3 points), 70% reduction in THI scores |
| Tinnitus suppression by intracochlear electrical stimulation in single-sided deafness - a prospective clinical trial: follow-upb | Arts R.A. et al | Quasi-experimental studies | 2015 | Multicentric | 10a | THI+TQ+VAS | SSD (moderate/severe) | 48.2 yr. | MED-EL, Concerto, OPUS2, Maestro version 4.1.2 | Unilateral | 1 to 12 | Reduction in THI scores (45 to 31 points), TQ (40 to 30 points) and VAS (7.1 to 2.8 points), 80% reduction in THI scores |
TQ, Tinnitus questionnaire; VAS, Visual qnalog scale; THI, Tinnitus handicap inventory; TRQ, Tinnitus reaction questionnaire.
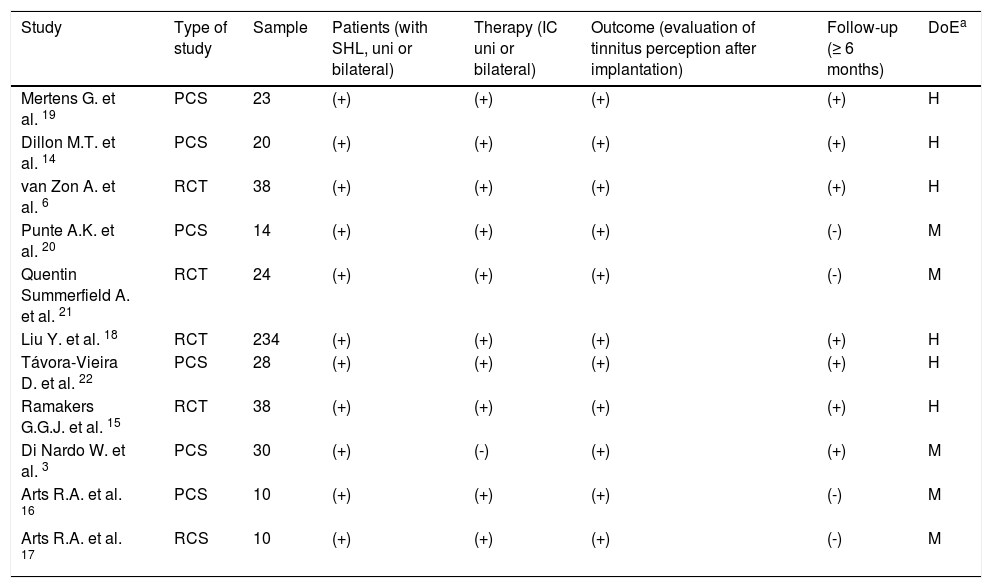
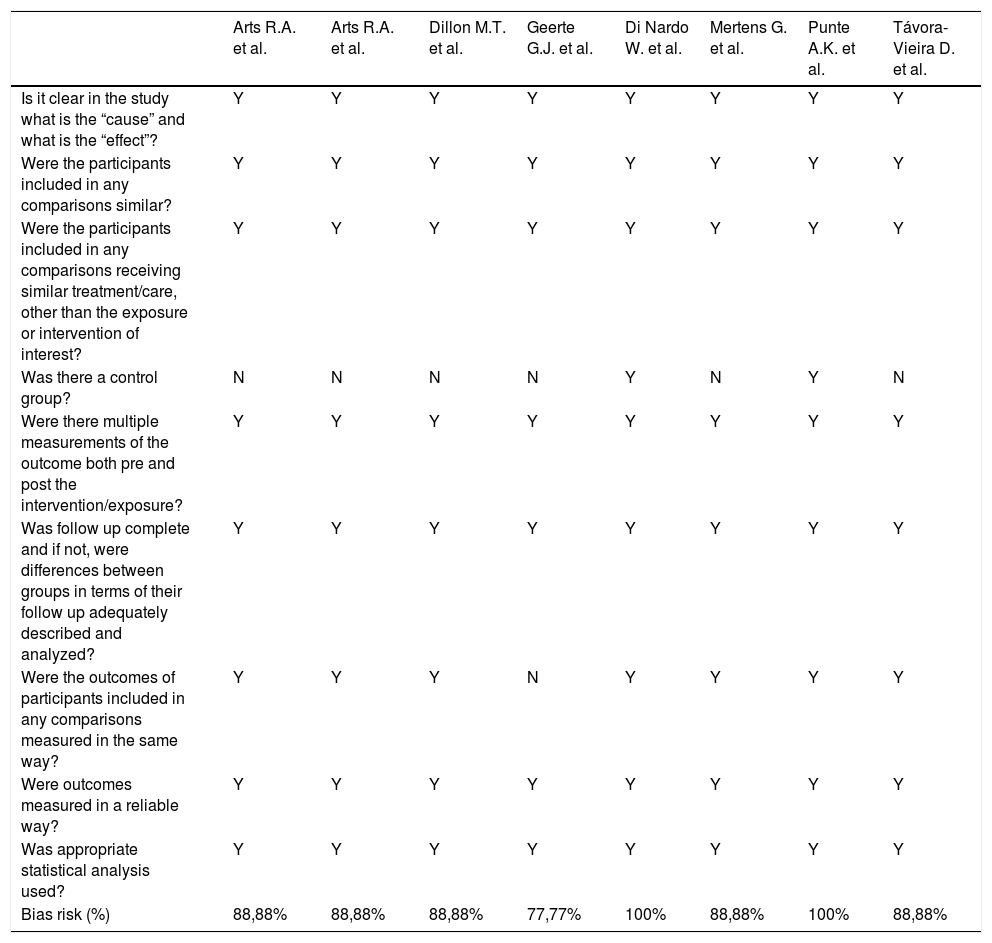
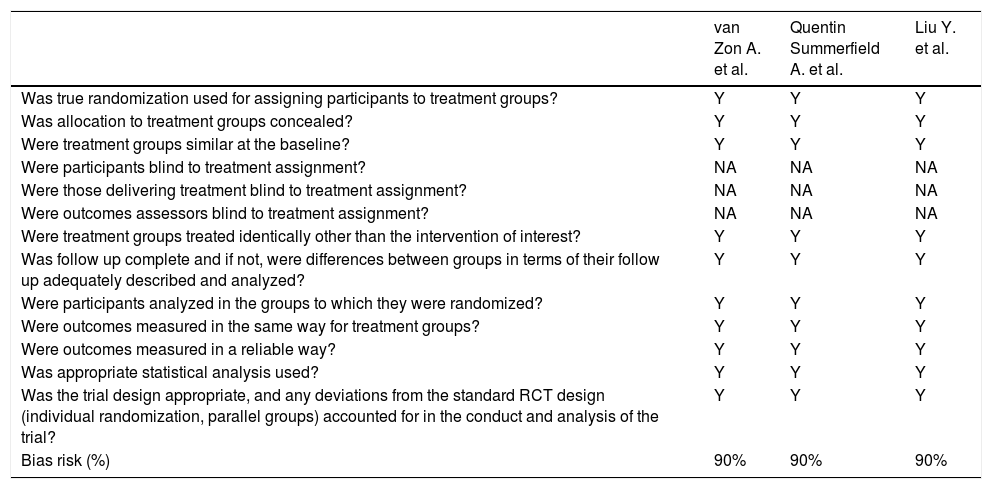
To assess the quality of the selected full-text studies, directness of evidence was evaluated according to the GRADE (grading of recommendations assessment, development and evaluation) approach outlined in the Cochrane handbook for systematic reviews of interventions, 17 which involved evaluations of the study population, therapy, and reported outcome. The criteria were adapted according to the study question and followed a similar structure as in the review by Ramakers et al. 14 High directness of evidence was defined as a positive score for all the criteria, moderate directness was recorded when the study met three out of the four criteria, and low directness of evidence was recorded when the study met fewer than three criteria (Table 2). The directness of evidence was found to be high in 6 studies 6,13,14,18–20 and moderate in 5 studies.3,15,16,21,22 None of these studies had a low directness of evidence. All the studies were prospective or retrospective case series. Risk of bias was assessed using the JBI critical appraisal checklist for quasi-experimental studies (Table 3) and the JBI critical appraisal checklist for randomized controlled trials (Table 4) according to the type of study, and all studies showed a low risk of bias.3,6,13–16,18–22
Quality Assessment of the studies based on directness category.
| Study | Type of study | Sample | Patients (with SHL, uni or bilateral) | Therapy (IC uni or bilateral) | Outcome (evaluation of tinnitus perception after implantation) | Follow-up (≥ 6 months) | DoEa |
|---|---|---|---|---|---|---|---|
| Mertens G. et al. 19 | PCS | 23 | (+) | (+) | (+) | (+) | H |
| Dillon M.T. et al. 14 | PCS | 20 | (+) | (+) | (+) | (+) | H |
| van Zon A. et al. 6 | RCT | 38 | (+) | (+) | (+) | (+) | H |
| Punte A.K. et al. 20 | PCS | 14 | (+) | (+) | (+) | (-) | M |
| Quentin Summerfield A. et al. 21 | RCT | 24 | (+) | (+) | (+) | (-) | M |
| Liu Y. et al. 18 | RCT | 234 | (+) | (+) | (+) | (+) | H |
| Távora-Vieira D. et al. 22 | PCS | 28 | (+) | (+) | (+) | (+) | H |
| Ramakers G.G.J. et al. 15 | RCT | 38 | (+) | (+) | (+) | (+) | H |
| Di Nardo W. et al. 3 | PCS | 30 | (+) | (-) | (+) | (+) | M |
| Arts R.A. et al. 16 | PCS | 10 | (+) | (+) | (+) | (-) | M |
| Arts R.A. et al. 17 | RCS | 10 | (+) | (+) | (+) | (-) | M |
DoE, Directness of evidence; H, High; M, Moderate; PCS, Prospective case series; RCS, Retrospective case series; RCT, Randomized Controlled Trial.
JBI Critical appraisal checklist for quasi-experimental studies.
| Arts R.A. et al. | Arts R.A. et al. | Dillon M.T. et al. | Geerte G.J. et al. | Di Nardo W. et al. | Mertens G. et al. | Punte A.K. et al. | Távora-Vieira D. et al. | |
|---|---|---|---|---|---|---|---|---|
| Is it clear in the study what is the “cause” and what is the “effect”? | Y | Y | Y | Y | Y | Y | Y | Y |
| Were the participants included in any comparisons similar? | Y | Y | Y | Y | Y | Y | Y | Y |
| Were the participants included in any comparisons receiving similar treatment/care, other than the exposure or intervention of interest? | Y | Y | Y | Y | Y | Y | Y | Y |
| Was there a control group? | N | N | N | N | Y | N | Y | N |
| Were there multiple measurements of the outcome both pre and post the intervention/exposure? | Y | Y | Y | Y | Y | Y | Y | Y |
| Was follow up complete and if not, were differences between groups in terms of their follow up adequately described and analyzed? | Y | Y | Y | Y | Y | Y | Y | Y |
| Were the outcomes of participants included in any comparisons measured in the same way? | Y | Y | Y | N | Y | Y | Y | Y |
| Were outcomes measured in a reliable way? | Y | Y | Y | Y | Y | Y | Y | Y |
| Was appropriate statistical analysis used? | Y | Y | Y | Y | Y | Y | Y | Y |
| Bias risk (%) | 88,88% | 88,88% | 88,88% | 77,77% | 100% | 88,88% | 100% | 88,88% |
JBI Critical appraisal checklist for randomized controlled trials.
| van Zon A. et al. | Quentin Summerfield A. et al. | Liu Y. et al. | |
|---|---|---|---|
| Was true randomization used for assigning participants to treatment groups? | Y | Y | Y |
| Was allocation to treatment groups concealed? | Y | Y | Y |
| Were treatment groups similar at the baseline? | Y | Y | Y |
| Were participants blind to treatment assignment? | NA | NA | NA |
| Were those delivering treatment blind to treatment assignment? | NA | NA | NA |
| Were outcomes assessors blind to treatment assignment? | NA | NA | NA |
| Were treatment groups treated identically other than the intervention of interest? | Y | Y | Y |
| Was follow up complete and if not, were differences between groups in terms of their follow up adequately described and analyzed? | Y | Y | Y |
| Were participants analyzed in the groups to which they were randomized? | Y | Y | Y |
| Were outcomes measured in the same way for treatment groups? | Y | Y | Y |
| Were outcomes measured in a reliable way? | Y | Y | Y |
| Was appropriate statistical analysis used? | Y | Y | Y |
| Was the trial design appropriate, and any deviations from the standard RCT design (individual randomization, parallel groups) accounted for in the conduct and analysis of the trial? | Y | Y | Y |
| Bias risk (%) | 90% | 90% | 90% |
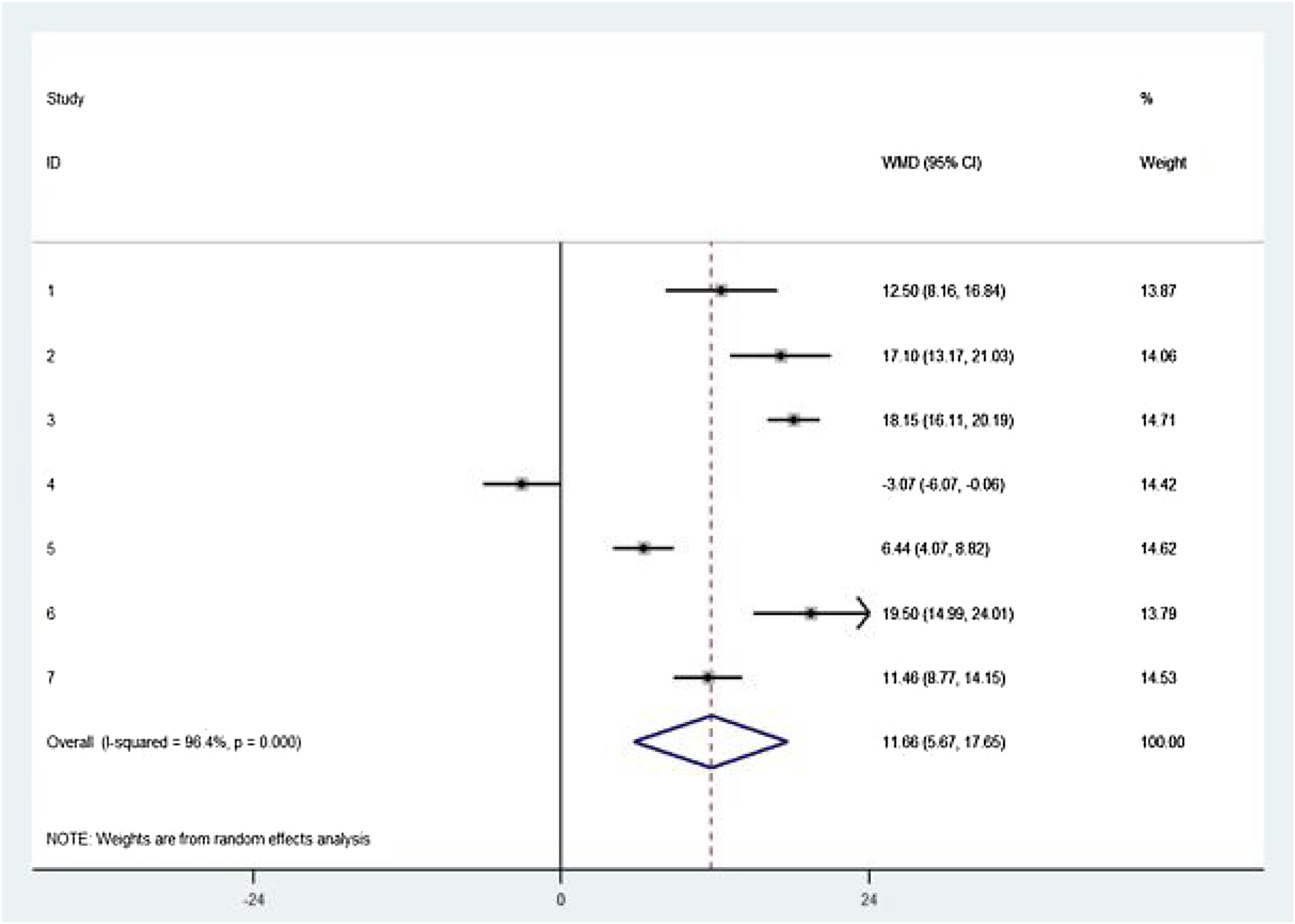
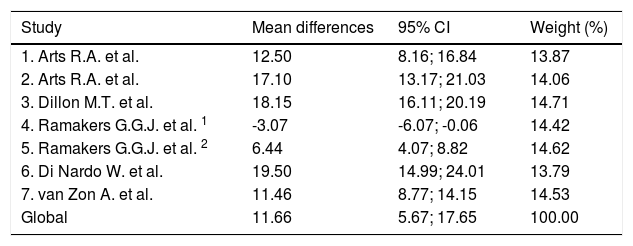
All 6 studies included in the meta-analysis evaluated tinnitus severity before and after cochlear implantation using the THI. The THI score was measured in 136 patients following cochlear implantation, with each patient's preoperative THI score used as the control. A statistically significant decrease in postoperative THI score was observed. A total decrease of 11.66 points in the THI score (95% CI 5.67 to 17.65; p<0.001) was observed after cochlear implantation, indicating a reduction in tinnitus severity. Marked heterogeneity was observed across the studies (I2=96.4%) (Table 5 and Fig. 2). The level of heterogeneity among the studies was assessed by I2. Because substantial heterogeneity was observed in the results of the various studies, the mean difference estimates were assessed using a random-effects model, enabling us to infer that the results of the meta-analysis are representative of the study population.
Meta-analysis estimates of cochlear implantation on the Tinnitus Handicap Inventory score. The mean summary difference across the studies indicated an 11.66-point reduction in the tinnitus severity score (95% CI 5.67 to 17.65; p<0.001). There was marked heterogeneity between the studies (I2=96.4%).
| Study | Mean differences | 95% CI | Weight (%) |
|---|---|---|---|
| 1. Arts R.A. et al. | 12.50 | 8.16; 16.84 | 13.87 |
| 2. Arts R.A. et al. | 17.10 | 13.17; 21.03 | 14.06 |
| 3. Dillon M.T. et al. | 18.15 | 16.11; 20.19 | 14.71 |
| 4. Ramakers G.G.J. et al. 1 | -3.07 | -6.07; -0.06 | 14.42 |
| 5. Ramakers G.G.J. et al. 2 | 6.44 | 4.07; 8.82 | 14.62 |
| 6. Di Nardo W. et al. | 19.50 | 14.99; 24.01 | 13.79 |
| 7. van Zon A. et al. | 11.46 | 8.77; 14.15 | 14.53 |
| Global | 11.66 | 5.67; 17.65 | 100.00 |
Heterogeneity (p-value<0.001); I2=96.4% of variation (randomized); global means test (p-value ≤ 0.001).

In the systematic review, all the articles showed an improvement in the perception of tinnitus, which is consistent with the results of other systematic reviews.23–25
DiscussionCochlear implant surgery has been used for auditory rehabilitation for years and has proven to be an important tool for improving the perception of tinnitus. Our meta-analysis and systematic review demonstrated that cochlear implantation leads to an improvement in tinnitus. We included patients who underwent unilateral and bilateral cochlear implantation, had bilateral hearing loss, presented with bilateral or unilateral tinnitus, and had single-sided deafness. We evaluated the results of cochlear implantation under a variety of situations and conducted a global analysis of the influence of cochlear implants on tinnitus.
Although many studies on tinnitus and its correlation with cochlear implantation have been conducted, the pathophysiologic mechanisms of tinnitus suppression after the procedure are not yet fully understood. A possible assumed explanation is that CI induces the restoration of central auditory pathways and induces neuroplasticity, which may affect tinnitus perception.18,19
In our meta-analysis, we observed considerable heterogeneity, which may be due to differences in the design of each study and in the characteristics of the participants of each study. The literature review yielded 11 studies; 5 studies analyzed patients with single side deafness (SSD), 1 evaluated patient with asymmetric hearing loss (AHL) and SSD, and 5 evaluated patients with bilateral loss. The follow-up time and follow-up procedures were different in each study. Two studies analyzed sequential and simultaneous implantation, but they used different intervals for the sequential implant.14,22 We standardized the meta-analysis with respect to the type of questionnaire applied to better assess the perception of tinnitus. The considerable heterogeneity observed in this study demonstrates that more studies should be conducted to determine the improvement in scores on standardized tests after implantation in this patient population. We decided to perform this meta-analysis, which showed high heterogeneity among the studies on this topic, as shown in the meta-analysis by Blasco et al., 23 which demonstrated a high degree of interstudy heterogeneity.
All the articles eligible for this meta-analysis reported an improvement in the perception of tinnitus, despite the differences in the parameters analyzed in each article. The study that analyzed simultaneous and sequential procedures for cochlear implantation 14 showed that the median decreases in tinnitus scores were equal after simultaneous and sequential bilateral implantation; there was an 8 point reduction in the median THI score and a 9 point reduction in the median TQ score. In the simultaneous group, tinnitus scores fluctuated in the 3 years after implantation.14 Another study that analyzed simultaneous procedures compared with unilateral procedures observed a significant decrease in tinnitus as measured by the THI in both unilaterally and bilaterally implanted patients, and there was a global reduction in the THI from 13 points to 3 points. In the bilaterally implanted patients, there was a significant decrease in the TQ score from 20 points to 9 points.6
Summerfield et al. 22 and van Zon et al. 6 observed in their study that there was no significant difference in tinnitus perception and newly induced perception after bilateral simultaneous cochlear implantation, sequential cochlear implantation or unilateral cochlear implantation. These findings reinforce the idea that cochlear implantation has a positive influence on tinnitus perception in both unilateral and bilateral procedures.
The majority of studies showed benefits in tinnitus perception after cochlear implantation, yet newly induced tinnitus was also reported in some studies. Therefore, all CI candidates should be informed about the risk of newly induced tinnitus, a possible complication.6
Studies that analyzed unilateral cochlear implantation in patients with SSD showed an important reduction in tinnitus perception.13,15,16,18,19,21 One study observed patients with SSD and AHL and found that there was a lower benefit in the TQ scores after cochlear implantation in the AHL group.18 These findings were probably related to improved hearing as the first primary benefit reported in the AHL group. However, that study showed short-term improvement in tinnitus perception and long-term stabilization in CI users.
Tinnitus perception worsened in few patients during the follow-up. The patients who showed great increases in tinnitus sensation in some studies probably had experience caused by chance, probably had different insertion depths of the electrode arrays, or probably had perception during one of the follow-up phases but was fixed for long-term improvement.18,19,21,22 Tinnitus is related to the steepness of hearing loss; if we electronically stimulate the basal area of the cochlea, it will reafferent the very high frequencies. Patients with high-frequency hearing loss and low frequencies showed no improvement in tinnitus perception after the activation of the basal electrodes.21 These findings suggest that the electrode insertion depth influences tinnitus improvement.
Although our work has high heterogeneity, the strengths of this study include the rigor of statistical testing and the number of subjects analyzed.
Studies eligible for systematic review also show an important reduction in the scores of various tinnitus questionnaires. Despite the positive results in improving tinnitus sensation after cochlear implantation, high-quality studies are required before standardizing cochlear implantation as a treatment for tinnitus in eligible patients with hearing loss.
Our meta-analysis revealed significant decreases in THI scores after cochlear implantation in patients with different types of hearing loss and at different lengths of follow-up. The high heterogeneity of analyzed parameters among the studies in this meta-analysis indicates a need for additional studies to establish cochlear implantation as a treatment for tinnitus. It is also necessary to develop studies to elucidate the mechanisms by which these improvements in tinnitus perception occur.
ConclusionPatients who experience preoperative tinnitus can benefit from either unilateral or bilateral cochlear implantation. All the patients in these studies showed improvements in the tinnitus perception score by more than 50% in the questionnaires performed.
Conflicts of interestThe authors declare no conflicts of interest.
Peer Review under the responsibility of Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial.


